
Policy Brief
Covid-19 prompts the EU and
theNetherlands to rethink
globalhealth
NOVEMBER 2021
Never waste a good crisis?
Global health revisited
In the wake of the Covid-19 pandemic,
global health policy has re-emerged on
the global political agenda. The European
Union (EU) and its member states have
increased their budgets, reflecting the
need for collective action to address the
pandemic. However, it is less clear to what
1 The authors are grateful for various review
comments by colleagues and external experts.
Funding for this publication was made available
by Cordaid, KNCVTBC and Aidsfonds. The content
falls under the responsibility of the authors only.
The Covid-19 pandemic prompted a strong re-engagement in global health.
Because the pandemic coincided with geopolitical rifts between the US and China,
but required a global response, the EU and its member states took responsibility to
safeguard the World Health Organization (WHO) and initiated global arrangements
for vaccine sharing for developing countries. Within the EU, mandates and global
health functions have traditionally been underdeveloped and divided between the
development and health sectors. For the Netherlands, this is perhaps the case to
an even larger extent. Development funding has focused primarily on sexual and
reproductive health and rights, and the health ministry has had limited interest and
capacity on international health issues, with the exception of certain specific issues
such as Anti-Microbial Resistance (AMR) and medicine prices. Spending on global
health by both the EU and the Netherlands has been fragmented, with mainly ad hoc
budgets being made available for the international pandemic response. This policy
brief calls for a structural response and more coherent outlook on global health.
extent the crisis has prompted structural
changes linked to a revision of global health
priorities and related financial investments
by the European Commission (EC) and the
Netherlands. For health ministries, the added
value of looking at health as a European and
international issue is not automatic. At the
same time, development actors seemed less
focused on public health security interests,
such as improving the early detection of
infectious diseases outbreaks or zoonotic
risks. Rather they focused more on other
issues such as universal health coverage.
This raises the question of what drives this
incoherent and weak profile of the EU and an
EU member state like the Netherlands in the
global health domain, and whether this will
be different now that the EU has experienced
Louise van Schaik, Martijn Haas and Remco van de Pas
1

2
Clingendael Policy Brief
the tremendous impacts of a pandemic.
What could be done to make the EU’s global
health efforts more coherent? And what
could the Netherlands contribute to a more
integrated EU approach?
Although the EU and its member states
are, in general, the largest provider of
development aid, the financial contributions
to global health have been relatively low
in comparison to other sectors.
2
From EU
member states, it is mainly Germany that is
a significant contributor in this field. This is
also apparent in funding for certain Covid-
related initiatives. For example, the European
Commission’s and EU member states’
collective pledge of over 2.5 billion USD to
the COVAX Advanced Market Commitment
(COVAX-AMC) was lower than the 3.3 billion
USD pledged by the US.
3
Moreover, the
funding is fragmented across many initiatives
targeting different aspects of the global
health agenda. This hinders the WHO’s role
as central coordination organisation in the
field of global health policy, even though
the funding from global health initiatives,
such as the Global Fund to Fight AIDS,
Tuberculosis and Malaria and the Global
Alliance for Vaccines and Immunization
2 Pauline Veron and Mariella Di Ciommo, Fit for
Purpose: The EU’s Role in Global Health in the Era
of COVID-19, 2020.
3 GAVI, Key Outcomes One World Protected - COVAX
AMC Summit: Assured Resources for the Gavi
COVAX AMC, 2021.
(GAVI), also pays for some WHO services
for implementing specific programmes.
Tensions over the initial handling by the
WHO of China’s response to the outbreak
of coronavirus exposed its vulnerability.
European countries and the EU stood up
to safeguard the WHO in response to the
US withdrawing its funding for the WHO.
The EU, moreover, initiated new global
responses, notably the COVAX facility
for joint purchases of vaccines.
4
Later on,
it proposed a pandemic treaty to prompt
a more coherent approach to pandemics
and prevent new outbreaks. It is not yet
clear how this new instrument links to the
International Health Regulations (2005),
which fall under the auspices of the
WHO and are meant to prompt pandemic
preparedness and responses.
Where is global health on
Europe’s agenda?
Health is perhaps one of the fields which
is least Europeanised, compared to, for
instance, economic, agricultural, trade and
environmental policies, where member
states are sharing more policy-making
4 Louise van Schaik, Knud Erik Jørgensen and
Remco van de Pas, ‘Loyal at once? The EU’s
global health awakening in the COVID-19
pandemic’, Journal of European Integration 42, no. 8
(16 November 2020): 1145–60.
Table 1 EU global health contributions in comparison
WHO (2018-2019) GAVI (2016-2020) Global Fund (2017-2019)
European Commission USD 131 million (2.33%) USD 243 million (3%) USD 532 million (4.7%)
US USD 893 million (15.88%) USD 1,400 million (15%) USD 3,718 million (32.6%)
UK USD 435 million (7.73%) USD 2,159 million (23%) USD 1,569 million (13.8%)
Germany USD 292 million (5.19%) USD 668 million (7%) USD 814 million (7.1%)
Netherlands USD 55 million (0.98%) USD 304 million (3%) USD 180 million (1.58%)
Sweden USD 77 million (1.37%) USD 198 million (2%) USD 293 million (2.57%)
Denmark USD 14 million (0.26%) USD 11 million (0%) USD 45 million (0.4%)
Source: WHO, Contributors (2018-2019), 2021; GAVI, Annual Contributions and Proceeds 30 June 2021, 2021;
the Global Fund, Data Explorer, 2021.
Note: The % figure relates to the states’ total share in the organisation’s budget

3
Clingendael Policy Brief
competences at EU level. This is also
reflected in the EU’s international outlook,
where (global) health has not featured
prominently in the past. In the European
Commission (EC) the Directorate-General for
International Partnerships (INTPA) and to a
lesser extent the Directorate-General (DG)
for Health and Food Safety (SANTE)
are in the lead for different aspects of
global health. Other DGs, including the
Research (RTD) and European External
Action Service (EEAS), are contributing to
specific aspects, such as funding global
health research and diplomacy efforts.
INTPA has just entered a new era after
the introduction of the Neighbourhood,
Development and International Cooperation
Instrument (NDICI) as main financial
instrument for development cooperation,
worth about 80 billion Euros in the period
2021-2027. Health is included under the
Social Inclusion heading and is traditionally
not a big item; nevertheless officers involved
in programming development funding
fear that budgets for health programmes
in partner countries are under pressure
because of the many competing demands for
NDICI funding. A limited amount of funding
for health is also available under the Global
Challenges heading of NDICI.
Within DG INTPA high hopes are on the
new ‘Team Europe’ approach, which would
encourage matched funding by the European
Commission and EU member states, thus
giving EU health programmatic support
and initiatives greater impact and visibility.
However, it remains to be seen whether this
approach will materialise in the field of global
health. Previous efforts to make EU efforts
more visible or to coordinate funding from
the EC and EU member states suffered from
a lack of interest by member states that had
their own development priorities. Moreover,
if national agendas or self-interest dominate
in Team Europe initiatives, the result might
be a development agenda that is less needs
based and coherent than is desirable.
INTPA is also in the lead regarding EU
support to the Global Fund, GAVI, COVAX,
the Global Financing Facility, etc. Here,
numbers have increased in recent years and
in response to the Covid-19 pandemic.
DG SANTE saw its budget for health security
increase by tenfold because of the pandemic,
but most of the funding will be spent within
the EU to new and revamped institutions
5
to address pandemics, develop treatment for
emerging infectious diseases and respond
adequately to epidemics early on. Together
with the European External Action Service
(EEAS) DG SANTE coordinates the EU’s
position in WHO. The direct budget from
the EU to WHO is limited, with the European
5 Examples are the European Centre for Disease
Prevention and Control (ECDC), European
Health Emergency Preparedness and Response
Authority (HERA), and the European Medicines
Agency (EMA).
Table 2 European Commission funding to global health initiatives
Current funding
(pledgesandcontributions)
Change since last funding period
CEPI (2020) USD 102 million (7,01%) + USD 5,8 million (2019)
COVAX AMC USD 489 million (4,98%) -
GAVI (2021-2025) USD 357 million (5,9%)* + USD 114 million (2016-2020)
Global Fund (2020-2022) USD 606 million (3,6%) + USD 73 million (2017-2019)
WHO (2020-Q2 2021) USD 576 million (6,36%) + USD 445 million (2018-2019)
Source: CEPI, 2020 Annual Progress Report, 2021; CEPI, 2019 Annual Progress Report, 2020; GAVI, Annual
Contributions and Proceeds 30 June 2021; the Global Fund, Data Explorer; WHO, Contributors (2018-
2019); WHO, Contributors (2020-2021), 2021; GAVI, Key Outcomes One World Protected - COVAX AMC
Summit: Assured Resources for the Gavi COVAX AMC.
* Excluding contributions and pledges to COVAX AMC, % figure relates only to total direct contributions
to GAVI.

4
Clingendael Policy Brief
Commission having contributed 131 million
USD to the WHO in the 2018/2019 biennium.
The contributions of the UK, US, Germany
and Japan surpassed the Commission’s
contribution to the WHO in recent years.
DG SANTE was also in the lead with regard
to the joint purchasing of vaccines for
the EU. A national focus in EU member
states at the start of the pandemic made
this vaccine sharing a difficult task, with
initiatives such as the ‘Inclusive Vaccine
Alliance’ initially undermining DG SANTE’s
efforts.
6
But eventually the EC, together
with negotiators from EU member states,
negotiated vaccine deals on behalf of the EU,
and this may be replicated in the future
for other disease outbreaks, including for
zoonotic diseases.
The efforts of DG INTPA and SANTE seem
only loosely connected and coordinated, and
this is also the case for the EU Council bodies
for which they develop legislative proposals
and common viewpoints. EU Council
Conclusions on global health of 2010 that
were adopted by development ministers of
EU members states quickly lost momentum.
This lack of coordination is related to the
absences of a common definition of global
health and EU objectives for global health.
Whereas DG INTPA focuses on health
from a development angle, emphasising
universal health coverage (UHC) and health
systems strengthening (HSS), DG SANTE
looks at health security requirements and
public health protection within the EU.
The compartmentalisation of different
aspects of global health and lack of joint
vision leads to a disconnect between the
EU’s internal and external approaches
to health, whereas pathogens, diseases,
medical products and services, and health
labour migrants travel across borders
transnationally.
6 Louise van Schaik and Remco Van de Pas,
Europeanising Health Policy in Times of
Coronationalism, Clingendael Policy Brief, 2020;
Jillian Deutsch and Sarah Wheaton, How Europe
Fell behind on Vaccines, Politico, 2021.
Dutch leadership on global
health narrowed down to sexual
and reproductive health rights
and AMR
The Dutch situation is somewhat similar to
that of the European Commission. In the
Netherlands global health policy is mainly
in the hands of the Ministry of Foreign
Affairs (MFA), or more specifically its DG on
International Cooperation (DGIS), and the
Ministry of Health (MoH).
With regard to development cooperation,
since the early 2010s a political choice has
been made in the Netherlands to focus
health spending on sexual and reproductive
health and rights (SRHR), as one of four
development spearheads.
7
It was considered
that on this issue a difference could be
made with programmes and political
and diplomatic efforts large enough to
have an impact in developing countries.
The policy includes combating maternal
mortality, treating HIV and AIDS and helping
LGBTI minorities.
It was soon realised that strengthening
health systems was a prerequisite for an
effective SRHR policy, and therefore some
support aimed to combine these two
fields. That choice has meant that very
little funding, capacity and expertise in
government and programmes is available
for other health topics. There is a clear
preference to fund efforts undertaken by
specific global health initiatives such as
the GAVI and the Global Fund. Parliament
generally favours these investments as they
are deemed to provide good value for money
on clearly defined objectives and indicators
for reporting on results.
Within the MoH, the international department
is a relatively small team with dedicated
staff focusing on WHO, EU health policy
and other international health policies.
The Netherlands has been an active
contributor to the Global Health Security
Agenda (GHSA), a US-initiated international
7 The others are food security, water and rule of law.

5
Clingendael Policy Brief
partnership to strengthen capabilities in the
field of health security. Dutch engagement in
the GHSA has focused on the risks of AMR
and supported a ‘One Health’ approach,
including mitigating the risks of zoonotic
diseases. In implementing the One Health
approach, the MoH also works with other
relevant ministries, for example the Ministry
of Agriculture. Another MoH priority has
been cooperation in seeking a reduction of
the price for (rare) medicines and recently
to promote local production of medicines.
Before and at the start of the Covid
pandemic, the higher echelons in the ministry
were focusing predominantly on national
health efforts. The EU’s joint purchasing of
vaccines was actively supported, but little
attention remained for other international
health questions.
The Dutch position in the WHO and
its contribution to health security in
countries outside the EU received little
attention in parliament either, except from
vaccine donations to specific countries,
for example Suriname and Indonesia.
8
In 2020, the International Advisory
Council on International Affairs (AIV)
was asked to quickly develop guidance
on how the Netherlands should respond
to the Covid - 19 pandemic internationally.
The resulting document recommended a
leading role for the EU in the pandemic
response and a bolstering of the WHO.
9
It pointed to the potentially devastating
impacts of the pandemic in developing
countries. In early 2021, the Dutch parliament
asked the AIV to prepare guidance on a
framework for the future Dutch Global Health
Strategy aimed at creating a more coherent
global health policy.
10
This advice might aid
a new government in formulating a new
approach to global health.
8 De Jonge, H M, Kamerbrief over Vaccindonatie,
2021.
9 Advisory Council on International Affairs,
Nederland En de Wereldwijde Aanpak van
COVID - 19, 2020.
10 Advisory Council on International Affairs,
Adviestraject Kaders Voor Een Nederlandse Global
Health Strategy, 2021.
Policy mandates and related networks
from the development and health side are
not well aligned when it comes to global
health. The focus on SRHR, including HIV
and AIDS, has resulted in a lack of attention
for supporting global health more generally
and has hampered a needs-based and
coherent global health approach, especially
in the context of the Covid-19 pandemic.
This is exemplified by the Inclusive Vaccine
Alliance (IVA) launched on 3 June 2020
and coordinated by the Netherlands MoH.
The IVA and its four member states aimed
to support Covid-19 vaccine research and
procurement. One day later, however, COVAX
was launched. COVAX has a similar aim to
the IVA but is a global effort launched by the
Coalition for Epidemic Preparedness (CEPI),
GAVI and the WHO. The Netherlands MFA
participated in the launch of COVAX but had
not communicated the launch of this flagship
global health project, which completely
overshadowed the IVA, to the MoH. This was
a surprising turn of events, since one of the
key roles of the MFA is to coordinate Dutch
contributions to international initiatives and
organisations such as the WHO and EU with
the respective experts of the international
department of the MoH.
Moreover, in 2020 the Netherlands
barely increased its funding to the WHO,
despite the latter being under pressure
by the US withdrawing its funds and
membership. It moreover became the
epicentre of Covid-19 surveillance, and
played a central role in sharing knowledge
and policy advice on how to handle the
Covid-19 pandemic.
6
Clingendael Policy Brief
Table 3 Dutch contribution to global health entities
(total share in organisation budget in brackets)*
COVAX AMC USD 83 million (0,84%)
GAVI (2021-2025)** USD 243 million (3%)
Global Fund (2020-2022) USD 114 million (2,14%)
WHO (2020-2021)*** USD 72 million (0,8%)
Source: WHO, Contributors (2020-2021); GAVI, Key Outcomes One World Protected - COVAX AMC
Summit: Assured Resources for the Gavi COVAX AMC; GAVI, Annual Contributions and
Proceeds 30 June 2021; the Global Fund, Data Explorer.
* Figures in brackets refer to the Dutch relative share in the organisation’s total budget.
** Excluding contribution to COVAX AMC. Includes period through 30 June 2021.
*** Data available up to Q2 2021.
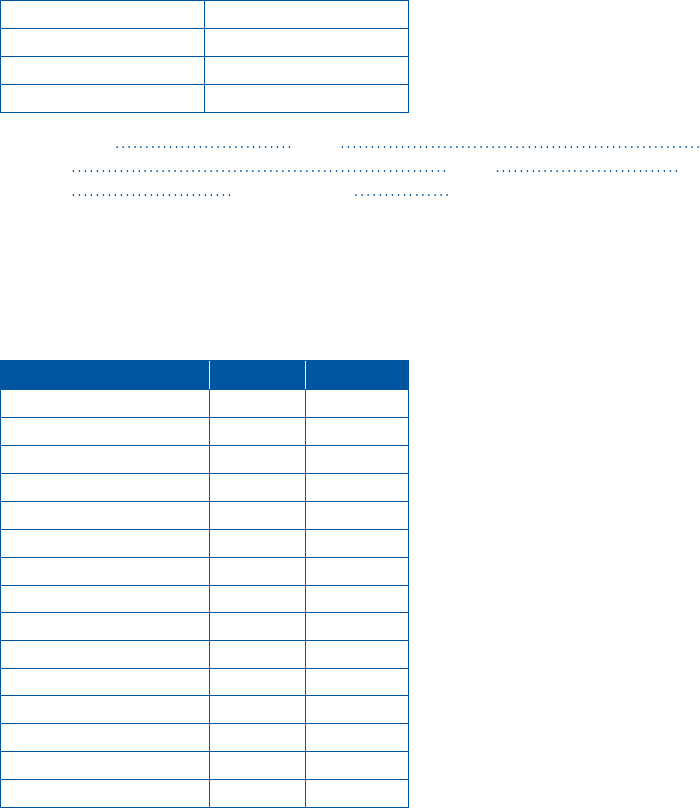
Table 4 Netherlands Ministry of Foreign Affairs global health spending
(in thousands)*
2019 2020
UN organisations
WHO 21.985 17.597
UNFPA 55.074 45.510
UNAIDS 10.000 30.000
UNICEF 12.000 7.000
Global health funds
GFF 14.859 16.114
G FATM 64.158 42.000
Gavi (incl. IFFIM) 52.121 44.467
Health Insurance Fund 10.090 10.030
Covid response
COVAX 0 5.000
GFF 0 10.000
FIND 0 5.000
Health Insurance Fund 0 7.500
* Data provided on request by the Netherlands Ministry of Foreign Affairs.
The MoH reduced its funding to the WHO
by €900.000 compared to 2019, and only
12.5 million euros were made available from
the MFA budget for the WHO’s role in the
Covid response. This is ad-hoc funding, and
on a structural basis the Dutch contribution
to WHO stayed at the same level, whereas
its contribution to global health initiatives
has been increasing (see overview). Only in
the autumn of 2021 was a new pledge made
of 95 million extra funding for Covid-related
global health investments, of which 30 million
will go to the WHO.
Another example of a global health initiative
falling out of the scope of the budgets of
both the MFA and the MoH is the European
and Developing Countries Clinical Trials
Partnership (EDCTP), which is an EU-African
global health research partnership based in
The Hague. The EDCTP played a key role in
the Covid-19 vaccine development process,
freeing up capacity for clinical trials of
Covid-19 vaccines with support from several
Dutch universities and non-governmental
organisations (NGOs). The Netherlands,
however, is reluctant to contribute to the next

7
Clingendael Policy Brief
funding cycle. The MoH considers the EDCTP
to be a development instrument, despite its
clear connection to health security, and the
MFA believes funding to EDCTP would fall
outside its mandate as it is not related to
SRHR. Although the Netherlands lobbied
hard to host the European Medicines Agency
in Amsterdam, it appears to have little
interest in funding the EDCTP.
The Dutch advocating for global
health in the EU?
With regard to the Dutch position in the
EU, the focus is on highlighting SRHR,
including HIV and AIDS, in EU policies
and programmes. Advocating for SRHR
has become more difficult because of
opposition by other EU member states to
SRHR policies that they consider inconsistent
with their socio-cultural values or religious
beliefs. SRHR is, however, Chefsache for the
Netherlands, and it is even prepared to block
EU Council decisions when SRHR language
is at risk of being deleted in relevant policies
and programmes. The Netherlands is also a
strong advocate of a Team Europe approach
to SRHR.
The focus on SRHR is, moreover, very
specific. For the Netherlands, SRHR is not
linked to demographic and population policy,
whereas it is linked in EC policy documents.
Population policy and reproductive health
for instance share a single category in EU
reports on external action financing. For the
EU, population growth is a recognised, albeit
contested, problem – with promotion of
women’s right to birth control being part of
the policy options for addressing it; but for
the Netherlands these two issues should not
be connected.
Apart from SRHR, the Netherlands is
not taking much interest in other health
spending in EU development programmes.
The Netherlands is also not overly active in
EU coordination with the WHO. This has to
do with its more general reluctance to the
Europeanisation of health policy, which is a
field where the EU only has a complementary
competence. The Netherlands is proud of
its relatively cost-effective national health
system and fears European interference
might compromise aspects of this system,
such as the mandatory social insurance
scheme that underpins it. There is a strong
reliance on national health institutions and
expertise. The WHO is considered one of
the sources of advice, but this has at times
been openly ignored, for instance on the use
of facemasks to prevent airborne infections.
Prime Minister Rutte signed a call pleading
for a pandemic treaty that was published
in major newspapers around the world, but
the issue has never been discussed in the
Dutch parliament.
11
Towards a more coherent Dutch
and EU policy on global health
Focus and generating impact seem to be
leading when it comes to choices made in
the field of global health by both the EU
and the Netherlands. This has been to the
detriment of placing policy choices in a
wider context and seeking alignment with
other priorities, such as strategic autonomy
or the European interests in addressing the
pandemic not only at home but also abroad.
The ‘rescue’ of the WHO, the initiation
of COVAX and current efforts to agree a
pandemic treaty are laudable, but a strategic
and coherent outlook on global health
governance is lacking. It is not clear if a
pandemic treaty would eventually fall under
the WHO’s institutional normative powers.
12
11 Bainimarama, J V et al., ‘COVID-19 Shows Why
United Action Is Needed for More Robust
International Health Architecture’ - Op-Ed Article
by President Charles Michel, WHO Director General
Dr Tedros Adhanom Ghebreyesus and More than
20 World Leaders, European Council, 2021.
12 Sridhar, D and Woods, N (2013). ‘Trojan
multilateralism: global cooperation in health’, Global
Policy, 4(4), 325-335.

8
Clingendael Policy Brief
In conclusion, a number of recommendations
can be made to global health policymakers.
European Commission:
• Consider the development of a new
global health strategy co-shaped by
development and health constituencies
in which a connection to global health
research and other related topics would
also be established. Organise a joint
meeting with health and development
ministers to adopt Council Conclusions
on the issue and set up a monitoring
mechanism and enhanced capacities
for following up on global health
commitments.
• Consider setting up a Team Europe
approach for global health, or subsets
such as pandemic response capabilities
or health-system strengthening in third
countries, to better align funding from
the European Commission and EU
member states. In this field, an effort led
by the European Commission is less likely
to bear fruit, as some EU member states
have a stronger signature in this field.
The Netherlands:
• Support the drafting and adoption of a
solid and integrated Dutch as well as
European global health strategy and
reconsider a more balanced Dutch
contribution, with increased attention
given to global public goods and needs-
driven global health issues.
• Further boost the capacity of the MoH
international department to improve its
handling of global health issues on EU
and WHO agendas. There has already
been an increase in the number of
staff, and it would be good if this was a
structural feature, rather than simply an
ad-hoc expansion of capacity related to
the Covid-19 pandemic.
Both the EU and the Netherlands have done
global health with a rather narrow mandate,
and it would be good if they become a
little less ‘Dutch’ on this policy challenge
and considered it in a more coherent and
structural way. A first step was made in
September 2021, when the Netherlands
MoH announced the donation of 27 million
vaccines to COVAX, matching the number of
vaccines already used in the Netherlands.
13
The MFA also announced new funding worth
€95 million euros to help fight the pandemic
in developing countries.
14
But most of the
Covid-related spending remains incidental,
and structural changes in funding priorities
in the wake of the pandemic are yet to be
discussed. If anything, the pandemic has
taught us that on this issue a more coherent
approach might be able to bring us more.
13 Rijksoverheid, Nederland Doneert 27 Miljoen
Vaccins Aan Covax, 2021.
14 Rijksoverheid, 95 Miljoen Euro Extra Voor
Coronabestrijding in Ontwikkelingslanden, 2021.

About the authors
Louise van Schaik is Head of Unit EU & Global Affairs at the
Clingendael Institute. Her research focuses on EU external action, global
health, climate change policy and a range of related topics.
Remco van de Pas is a public health doctor and a global health
researcher. He is a Senior Research Associate at the Clingendael
Institute, Senior Research Fellow Global Health Policy at the Institute of
Tropical Medicine, Antwerp and a lecturer in Global health at Maastricht
University.
Martijn Haas is a Research Assistant in the EU & Global Affairs Unit of
the Clingendael Institute.
About the Clingendael Institute
Clingendael – the Netherlands Institute of International Relations –
is a leading think tank and academy on international affairs.
Through our analyses, training and public debate we aim to inspire
and equip governments, businesses, and civil society in order to
contribute to a secure, sustainable and just world.
www.clingendael.org @clingendaelorg
info@clingendael.org The Clingendael Institute
+31 70 324 53 84 The Clingendael Institute
clingendael_institute
Clingendael Institute
Newsletter
