Data De-Identification
Guidelines (DDG)
California Health and Human Services
September 23, 2016
Version 1.0
CHHS Data De-Identification Guidelines (DDG) Page 2 of 68
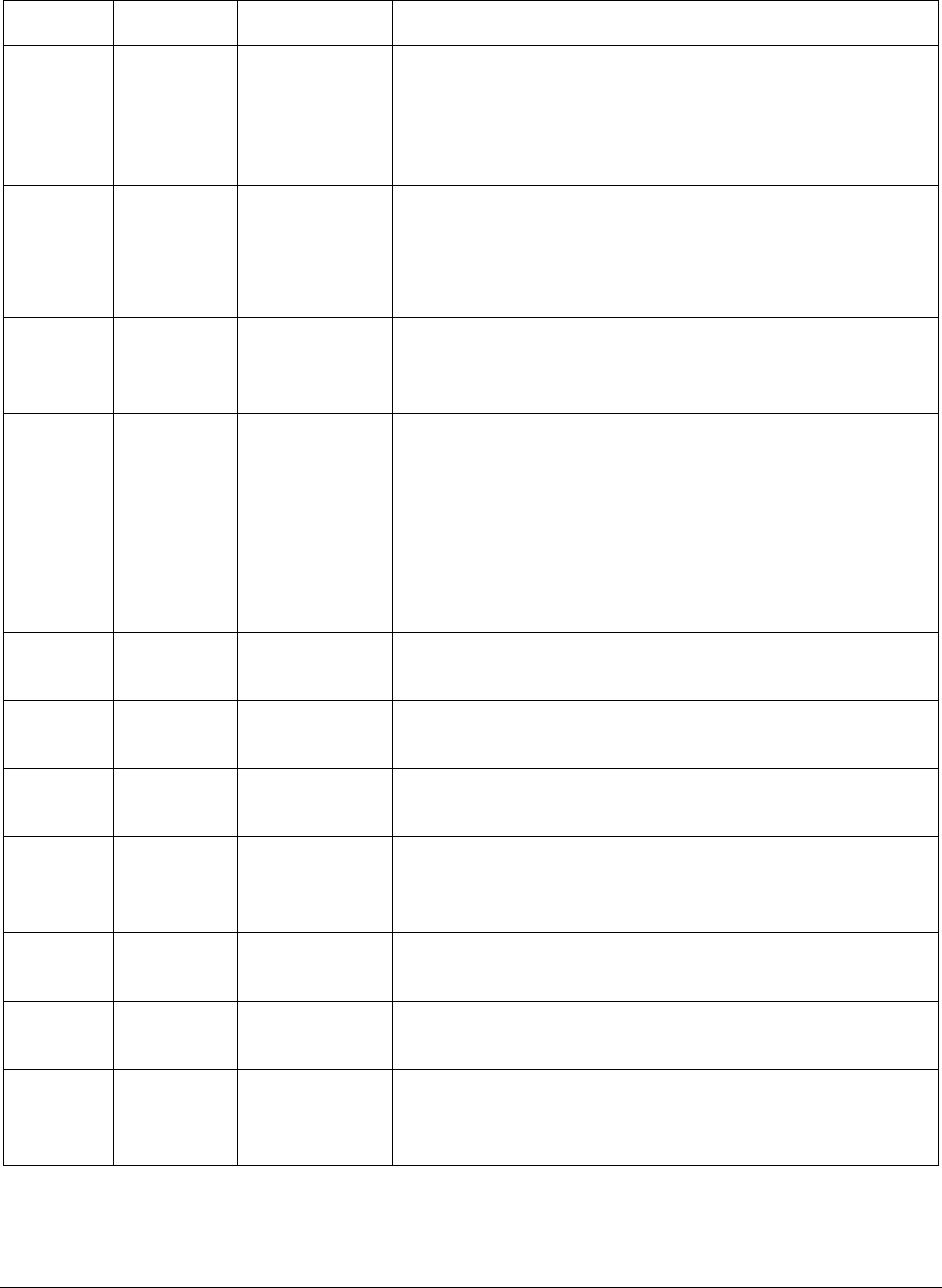
Revision History
Version
Date
Author
Brief Description of Changes
0.1
5/26/15
L. Scott
Initial draft for review which was based on the
DHCS PAR-DBR Guidelines dated 8/25/14 and
conversations at the CHHS Data De-
identification Workgroup meetings.
0.2
6/29/15
L. Scott
Additions made based on feedback:
CHHS Data De-identification Workgroup
meetings on May 27, 2015 and June 8, 2015
Department specific meetings
0.3
8/5/15
L. Scott
Additions and changes based on feedback from
all departments with specific written comments
from CDPH, OSHPD, DCSS, CDSS, MHSOAC.
0.4
1/22/16
L. Scott
Revisions based on recommendations from:
NORC
CHHS DDG Workgroup
CHHS Risk Management Subcommittee and
associated Legal and Privacy Workgroup
Specific written comments from CDPH,
CDSS
0.5
3/18/16
L. Scott
Revisions based on comments from CDPH,
CDSS, OSHPD, DHCS.
0.6
4/4/16
L. Scott
Revisions based on feedback from and
discussion with the Data Subcommittee
0.7
5/3/16
L. Scott
Revisions based on feedback from and
discussion with the Data Subcommittee
0.8
6/17/16
L. Scott
Revisions based on direction from the CHHS
Governance Advisory Council and input from the
CHHS Risk Management Committee
0.9
7/5/16
P. Cervinka
Revisions based on clarification from the CHHS
Governance Advisory Council
0.10
7/11/16
L. Scott
Formatting and citations edits to be consistent
with previous version 0.8
1.0
9/23/16
L. Scott
Revisions based on direction from the CHHS
Undersecretary. Approved as Version 1.0 for
implementation.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 3 of 68
Table of Contents
1) Purpose .................................................................................................................... 5
2) Background .............................................................................................................. 5
3) Scope ....................................................................................................................... 6
4) Statistical De-identification ..................................................................................... 11
4.1 Personal Characteristics of Individuals ............................................................ 15
4.2 Numerator – Denominator Condition ................................................................ 15
4.3 Assess Potential Risk ....................................................................................... 16
4.4 Statistical Masking ........................................................................................... 19
4.5 Legal Review .................................................................................................... 20
4.6 Departmental Release Procedure for De-identified Data ................................. 20
5) Types of Reporting ................................................................................................. 21
5.1 Variables .......................................................................................................... 21
5.2 Survey Data ..................................................................................................... 22
5.3 Budgets and Fiscal Estimates .......................................................................... 23
5.4 Facilities, Service Locations and Providers ...................................................... 23
5.5 Mandated Reporting ......................................................................................... 24
6) Justification of Thresholds Identified ...................................................................... 25
6.1 Establishing Minimum Numerator and Denominator ........................................ 25
6.2 Assessing Potential Risk – Publication Scoring Criteria ................................... 26
6.3 Assessing Potential Risk – Alternate Methods ................................................. 37
6.4 Statistical Masking ........................................................................................... 38
7) Approval Processes ............................................................................................... 41
8) DDG Governance ................................................................................................... 44
9) Publicly Available Data ........................................................................................... 45
10) Development Process ......................................................................................... 48
11) Legal Framework ................................................................................................. 50
12) Abbreviations and Acronyms ............................................................................... 60
13) Definitions ............................................................................................................ 61
14) References .......................................................................................................... 62

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 4 of 68
15) Appendix A: Expert Determination Template ....................................................... 65
16) Appendix B: 2015 HIPAA Reassessment Results ............................................... 66
17) Appendix C: State and County Population Projections ........................................ 67

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 5 of 68
1) Purpose
The California Health and Human Services Agency (CHHS) Data De-identification
Guidelines (DDG) describes a procedure to be used by departments and offices in the
CHHS to assess data for public release. As part of the document, specific actions that
may be taken for each step in the procedure are described. These steps are intended
to assist departments in assuring that data is de-identified for purposes of public release
that meet the requirements of the California Information Practices Act
1
(IPA) and the
Health Insurance Portability and Accountability Act
2
(HIPAA) to prevent the disclosure of
personal information.
Additionally, the DDG support CHHS governance goals to reduce inconsistency of
practices across departments, align standards used across departments, facilitate the
release of useful data to the public, promote transparency of state government, and
support other CHHS initiatives, such as the CHHS Open Data Portal.
2) Background
CHHS implemented an agency-wide governance structure in October, 2014. The
governance structure acts both in a decision-making and advisory capacity to Agency
leadership and its departments and offices. Implementation of the governance
framework supports information technology (IT) initiatives that are more tightly aligned
with meeting business objectives, enhanced project prioritization and improved strategic
IT investment decisions. The Executive Sponsor is the Undersecretary of CHHS. The
Advisory Council consists of representatives of senior leadership from departments and
offices in the Agency. There are five subcommittees that report to the Advisory Council,
which include the Portfolio, Procurement, Infrastructure, Risk Management and Data
Subcommittees. The Data De-identification Workgroup was convened by the Data
Subcommittee with representation from all departments and offices in CHHS.
CHHS is engaged in improving transparency and public reporting through the Open
Data Portal. As described in the CHHS Open Data Portal Handbook, not all data is
suitable for use on the open data portal. Data is Publishable State Data if it meets one
of the following criteria: (1) data that are public by law such as via the Public Records
Act
3
(PRA) or (2) the data are not prohibited from being released by any laws,
regulations, policies, rules, rights, court order, or any other restriction. Data shall not be
1
Civ. Code § 1789 et seq.
2
HIPAA Privacy Rule is located at 45 CFR Part 160 and Subparts A and E of Part 164
3
Gov. Code 6250 et seq.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 6 of 68
released if it is restricted due to the HIPAA, state or federal law. Data tables may fall
into one of three categories:
4
Level One: Data tables that can be released to the public and published without
restriction;
Level Two: Data tables that have some level of restriction or sensitivity but
currently can be made available to interested parties with a signed data use
agreement; or
Level Three: Level three data are restricted due to HIPAA, state or federal law.
These data will NOT be accessible through the CHHS Open Data Portal.
Data can change from being Level 3 to Level 1 if appropriate de-identification processes
are employed. The CHHS DDG described in this document will support departments
and offices in the evaluation of data to determine whether it has been adequately de-
identified so that it can be considered Level 1.
3) Scope
Data de-identification practices will be implemented by each department and office
(further referred to as department) in the agency. This DDG is the default policy for
CHHS departments. If a CHHS department wants to create a department DDG, it must
have appropriate references to departmental processes and the department must file a
copy of their DDG with the Office of the Agency Information Officer (OAIO). For
example, the Legal Review process and the Departmental Release Procedures for De-
Identified Data require additional information to describe these steps within each
department. Additionally, a department with programs not covered by HIPAA will not
require specific HIPAA references. A department must request DDG consultation from
the CHHS peer review team (PRT), described in Section 8: DDG Governance prior to
implementation. The PRT is available to review the department’s documentation to
ensure it is consistent with the principles of the CHHS DDG and meets requirements of
the California IPA.
The CHHS DDG is focused on the assessment of aggregate or summary data for
purposes of de-identification and public release. Aggregate data means collective data
that relates to a group or category of services or individuals. The aggregate data may
be shown in table form as counts, percentages, rates, averages, or other statistical
groupings.
4
CHHS’ Open Data Portal Handbook, Version 2.1, October 2014, Data Levels Decision Tree, pages 91
and 92.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 7 of 68
Departments are sometimes asked to release record level data. Record level data
refers to information that is specific to a person or entity. For example, a record for
Jane Doe may include demographics and case information specific to Jane Doe.
However, summary data would include information from Jane Doe combined, or
summarized, with data from other individuals. If record level data is to be publicly
released, it must be assessed to ensure it is de-identified and does not include Personal
Information (PI)
5
or Protected Health Information (PHI).
6
Although the DDG is focused
on summarized data, it can be used to assist with review of individual or record level
data. The record level data should be assessed both for uniqueness of the records and
for the possibility that the data can be used in conjunction with other information
available to the requester to identify individuals in the data. Record level data inherently
has higher risk than summarized data, even after personal identifiers are removed.
Therefore, record level data for public release should be assessed on a case by case
basis.
CHHS collects, manages and disseminates a wide range of data. The focus for the
DDG is on data that includes personal characteristics of individuals who have a legal
right to privacy. Personal characteristics include but are not limited to age, race, sex,
and residence and other identifiers specified in the IPA and HIPAA and listed in Figure
1. These guidelines will focus on the assessment of personal characteristics that are
included in various data sets or tables to assess risk for identification of the individuals
to which they pertain.
5
Personal Information is defined by California Civil Code section 1798.3 and Government Code section
11015.5.
6
“PHI” is defined as information which relates to the individual’s past, present, or future physical or
mental health or condition, the provision of health care to the individual, or the past, present, or future
payment for the provision of health care to the individual, and that identifies the individual, or for which
there is a reasonable basis to believe can be used to identify the individual. (45 CFR section 160.103)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 8 of 68
Figure 1: Unique Identifiers
CA – Personal Information
HIPAA – Safe Harbor (PHI)
Any information that
identifies or describes an
individual, including but not
limited to:
7
Name
Social security number
Physical description
Home address
Home telephone number
Education
Financial matters
Medical history
Employment history
Electronically collected
personal information:
8
his or her name
social security number
physical description
home address
home telephone number
education
financial matters
medical or employment
history
password
electronic mail address
information that reveals
any network location or
identity
Excludes information relating
to individuals who are users
serving in a business
capacity, including, but not
limited to, business owners,
officers, or principals of that
business.
Names
All geographic subdivisions smaller than a state,
including street address, city, county, precinct, ZIP
code, and their equivalent geocodes, except for the
initial three digits of the ZIP code if, according to the
current publicly available data from the Bureau of the
Census:
- The geographic unit formed by combining all ZIP
codes with the same three initial digits contains
more than 20,000 people; and
- The initial three digits of a ZIP code for all such
geographic units containing 20,000 or fewer
people is changed to 000
All elements of dates (except year) for dates that are
directly related to an individual, including birth date,
admission date, discharge date, death date, and all
ages over 89 and all elements of dates (including
year) indicative of such age, except that such ages
and elements may be aggregated into a single
category of age 90 or older
Telephone numbers
Fax numbers
Email addresses
Social security numbers
Medical record numbers
Health plan beneficiary numbers
Account numbers
Certificate/license numbers
Vehicle identifiers and serial numbers, including
license plate numbers
Device identifiers and serial numbers
Web Universal Resource Locators (URLs)
Internet Protocol (IP) addresses
Biometric identifiers, including finger and voice prints
Full-face photographs and any comparable images
Any other unique identifying number, characteristic,
or code
7
California Civil Code 1798.3 (a)
8
California Government Code 11015.5 (d) (1)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 9 of 68
Assessing the risk of an unauthorized disclosure that violates an individual’s right to
privacy and/or confidentiality, as provided by statute, may be achieved by associating
personal characteristics with a person’s identity or attributes. When these
characteristics can successfully confirm an individual’s identity in a publicly released
data set, then release of this data results in disclosure of personal information.
Less obvious qualities in data sets and elements that may be used to identify individuals
or groups can present uniqueness in data. Individual uniqueness in the released data
and in the population is a quality that helps distinguish one person from another and is
directly related to re-identification of individuals in aggregate data. Disclosure risk
becomes a concern when released data reveal characteristics that are unique in both
the released data and in the underlying population. The risk of re-identifying an
individual or group of individuals increases when unique or rare characteristics are
“highly visible”, or are readily accessible by the general public without any special or
privileged knowledge. Unique or rare personal characteristics (e.g., height above 7 feet)
or information that isolate individuals to small demographic subgroups (e.g., American
Indian Tribal membership) increase the likelihood that someone can correctly attribute
information in the released data to an individual or group of individuals.
9
Assessment of variables and their uniqueness
There are a number of variables that are unique to individuals that have been identified
in various laws and are considered identifiers (PI/PHI). There are two primary laws that
describe identifiers, shown in Figure 1, in California: the IPA and the federal HIPAA.
Other variables that are commonly used to publish information to the public have been
called quasi-identifiers because while they are not unique by themselves, they can
become unique in the right combination. The variables shown in the Publication
Scoring Criteria in Figure 6 can be considered quasi-identifiers and will be discussed
further in Sections 4 and 6.
Assessment of risk in the context of maximizing the usefulness of the information
presented
The removal of PI and PHI from datasets is often considered straight-forward, because
as soon as data is aggregated or summarized the majority of the data fields defined as
identifiers in the IPA and HIPAA are removed. However, various characteristics of
individuals may remain that alone or in combination could contribute to identifying
individuals. These characteristics have been described as quasi-identifiers. Figure 2
helps demonstrate the quasi-identifier concept. For instance, there is interest in
reporting about providers, where providers may be individuals, clinics, group homes, or
other entities. Each of these providers has a publicly available address and has publicly
9
Introduction to Statistical Disclosure Control, Temple et al. 2014

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 10 of 68
available characteristics. While patients may come to a provider from anywhere, they
typically will visit providers within a certain distance of their residence. Thus, by publicly
publishing details on providers, data miners with malicious intent would have a targeted
geography that lists locality information, types of services offered and received, and
demographic information about patients. To expand on this example, data that states a
provider saw two patients with heart disease does not indicate who had the heart
disease nor does it reveal the identity of the two patients amongst the thousands of
patients that provider sees. However, datasets that display a provider within a given
region with two Black or African American female patients under age 10 with heart
disease may release enough personal characteristics about the patients to successfully
reveal their identity. These compounding patient details released about providers that
give geography information (address), health condition (heart disease), and person-
based characteristics (quasi-identifiers) of the patients puts the dataset in the
overlapping area of the diagram of Figure 2. This overlap, consequently, highlights
potential risks associated with seemingly innocent summary data.
Figure 2: Relationship of Types of Reporting Variables
Health and Human Services
Utilization Data
(visits, diagnoses,
services, etc.)
Providers
(Individuals, Hospitals,
Clinics, Plans, Foster Care
Homes, etc.)
Provider
Performance
Personal
Characteristics
(IPA Identifiers (PI),
HIPAA Identifiers (PHI),
quasi-identifiers)
PI/PHI
PI/PHI
PI/PHI

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 11 of 68
4) Statistical De-identification
The DDG describes a procedure, the Data Assessment for Public Release Procedure
shown in Figure 5, to be used by departments in the CHHS to assess data for public
release. This section, section 4, describes specific actions that may be taken for each
step in the procedure with additional supporting information being described in sections
5, 6 and 7. These steps are intended to assist departments in assuring that data is de-
identified for purposes of public release that meet the requirements of the California IPA
to prevent the disclosure of personal information.
The Data Assessment for Public Release Procedure includes the following steps:
1. Review the data to determine if it includes personal characteristics, directly or
indirectly, that can be tied back to an individual;
2. If there is concern for personal characteristics, then assess the data for small
numerators or denominators;
3. If there is concern for small numerators or denominators, assess potential risk of
data release;
4. If there is potential risk identified, assess the need to apply statistical masking
methods to de-identify the data;
5. Following statistical de-identification, the data release is reviewed by legal if
indicated in departmental procedures; and,
6. After statistical de-identification, the data is reviewed and approved for release
based on program and policy criteria pursuant to departmental procedures.
The steps above are represented in a step-wise process shown in Figure 5. Each step
is described in further detail in section 4.1 through 4.6.
Data summaries that originate from data which includes personal identifiers must be de-
identified before release to the public. Additionally, data summaries about conditions
experienced by individuals must be adequately de-identified to prevent re-identification
of individuals represented by the summarized data. Various statistical methods are
available to statistically de-identify data.
Summarized data may be reviewed in the context of the numerator and the denominator
for the given presentation. The numerator represents the number of events being
reported while the denominator represents the population from which the numerator is
taken. For example, if it is reported that there are 50 cases of diabetes in California
then the numerator would be the number of cases (50) and the denominator would be
the number of people in California that could have diabetes (more than 38 million
people since diabetes can occur at any age or sex). While the numerator is relatively

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 12 of 68
straight-forward to identify, the denominator can be difficult. Data summaries are
frequently presented in tables in which numerators and denominators may be identified.
The numerator is typically the value in each table cell. However, the denominator can
be difficult to identify given the various ways in which tables are prepared. Two
examples of tables, Figure 3 and Figure 4, show the numerators and denominators in
sample tables.
Figure 3 shows an example table with the numerator and the denominator highlighted.
The Cells in the table are the boxes with values in them, as opposed to the row and
column headings. The row headings are 2012 and 2011. The column headings are
Year, # of Medi-Cal Members in Fee For Service (in thousands) and Number of Medi-
Cal Members in Managed Care (in thousands). In Figure 3, “2,775” is the value in a
table cell and represents a numerator. The sum of the row for year 2012 (2,775 + 4,853
= 7,628) represents a denominator. In this context, the denominator may represent row
totals, column totals or the total occurrences in the data set released. Data in Figure 3
comes from the “Trend in Medi-Cal Program Enrollment by Managed Care Status - for
Fiscal Year 2004-2012, 2004-07 - 2012-07.”
10
Figure 4 shows another type of table that contains rates. In this case, the numerator is
the number of Salmonella cases for a sample of California Local Health Jurisdictions in
2014. The table also includes the rate of Salmonella for these jurisdictions. In order to
10
Report Date: July 2013
http://www.dhcs.ca.gov/dataandstats/statistics/Documents/1_6_Annual_Historic_Trend.pdf
Figure 3: Illustration of numerators and denominators in a table.
Year
# of Medi-Cal Members
in Fee For Service
(in thousands)
# of Medi-Cal Members
in Managed Care
(in thousands)
2012
2,775
4,853
2011
3,067
4,527
Numerator
# of Medi-Cal Members in Fee For
Service (in thousands)
2,775
Denominator
# Medi-Cal Members in 2012
(in thousands)
7,628
Row Headings
Table Cell
Column
Headings

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 13 of 68
calculate the rate, the population size of each jurisdiction is required, but is not shown
directly in this table. The population denominator is an important element for data de-
identification.
Figure 4: Illustration of Numerators and Denominators in a Table of Rates

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 14 of 68
Step 2 –Numerator – Denominator Condition
Are the numerators (table cells) derived from fewer than 11 individuals OR
the denominators for the numerators less than 20,000 individuals?
If Yes, Go to Step 3 If No, Go to Step 5
Step 3 – Assess Potential Risk
Use a documented method to assess risk that small numerators or
small denominators may result in conditions that put individuals at
risk of being re-identified. Is there potential risk?
If Yes, Go to Step 4 If No, Go to Step 5
Step 6 – Departmental Release Procedures for De-Identified Data
After completion of the statistical de-identification process, each department will
specify the additional review steps necessary for public release of various data
products. Products may include but are not limited to reports, presentations, tables,
PRA responses, media responses and legislative responses.
Step 5 – Legal Review
Necessity of criteria for this step will be determined by each department. This
may vary depending on the purpose of the release and whether or not the
department/program is a HIPAA covered entity.
Step 4 –Statistical Masking
Assess the need to apply statistical masking methods to de-
identify the data. Use documented processes to apply
statistical masking that mitigates potential risk.
Figure 5: Data Assessment for Public Release Procedure
NO
NO
YES
YES
YES
NO
Step 1 – Personal Characteristics of Individuals
Does data provide personal characteristics (directly or indirectly) of individuals
that is not expressly allowed to be released publicly (eg. Provider data)?
If Yes, Go to Step 2 If No, Go to Step 6
Statistical
Data De
-identification Assessment
Review and Release

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 15 of 68
4.1 Personal Characteristics of Individuals
As described in Section 3 and Figure 2, personal characteristics of individuals introduce
the most significant risk with respect to identifying individuals in a data set. The
following are examples of personal characteristics.
Identifiers as defined in CA IPA
Identifiers as defined in HIPAA
Demographics typically reported in census and other reporting
o Race
o Ethnicity
o Language Spoken
o Sex
o Age
o Socio-economic status as percent of poverty
Personal characteristics are those characteristics that are distinctive to a person and
may be used to describe that person. Personal characteristics include a broader set of
information than those data elements that may be specifically defined as identifiers
(such as, driver license, address, birth date, etc.). Personal characteristics may also be
inferred from characteristics related to provider or utilization data. For example, if
presented with information about a provider that only sees women, it can be inferred
that the clients are women even if that is not specifically stated in the data presentation.
4.2 Numerator – Denominator Condition
The Numerator – Denominator Condition represents a combination of both the
Numerator Condition and Denominator Condition and for which both conditions must be
met or else a more detailed assessment is required. This may be considered as an
initial screening of a data set.
Numerator – number of events with the characteristics of the given row and column
Denominator – the population from which the events arise
The Numerator Condition sets a lower limit for the cell size of cells displayed in a table.
The DDG has set this limit as any value representing aggregated or summarized
records which are derived from less than 11 individuals (clients). Of note, values of
zero (0) are typically shown since a non-event cannot be identified.
The Denominator Condition sets a minimum value for the denominator. The DDG has
identified the lower limit for the denominator to be a minimum value of 20,000.
Since this is a Numerator – Denominator Condition, both the minimum cell size for the
numerator and denominator must be met. If these conditions are met, the table can

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 16 of 68
move to Step 5 for consideration for release to the public. If either the numerator of
denominator condition is not met, then the review of the data must proceed to Step 3.
4.3 Assess Potential Risk
This step requires the use of a documented method to assess the risk that small
numerators or small denominators may result in conditions that put individuals at risk of
being re-identified.
Assessment of potential risk for a given data set must take into account a range of
contributing considerations. This includes understanding particular characteristics of a
given data set that is being released. For example, if the potential values for a specific
personal characteristic, such as race, results in many small numbers in data set A but
does not in data set B, then the risk may be low for data set B and high for data A if the
groupings of the personal characteristics include the same categories. For this reason,
each department or program may set different values for risk based on the underlying
distribution of these variables in the data sets of interest.
There are many methods used to assess potential risk. Many of the methods that are in
use throughout the country are described in the various references provided in Section
15. While each department will document the method(s) chosen for use, the following
description of the Publication Scoring Criteria is provided as an example and may be
adopted by departments as a method to assess potential risk.
Publication Scoring Criteria: Example of tool to assess potential risk
The Publication Scoring Criteria is used to identify the presence of small values that are
considered sensitive in order to facilitate the assessment of potential risk. The
Publication Scoring Criteria combines a number of conditions that increase the risk of a
given data table and allows the department to evaluate those risks in combination with
each other. The variables included in the Publication Scoring Criteria are those
variables routinely used to publish data but are not all inclusive.
A variable is a symbol representing an unknown numerical or categorical value in an
equation or table. A given variable may have different ranges assigned to it. Ranges
assigned to the variable may be defined many ways which may increase or decrease
the risk of identification of an individual represented in the table. This is seen in the
Publication Scoring Criteria in that ranges for variables which will produce smaller
groupings have a higher score.
The Publication Scoring Criteria in Figure 6 quantifies with a score two identification
risks: size of potential population and variable specificity. The Publication Scoring
Criteria is used to assess the need to perform statistical masking as a result of a small
numerator, small denominator, or both. The Publication Scoring Criteria takes into

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 17 of 68
account both variables associated with numerators, such as Events, and with
denominators, such as Geography.
This method requires a score less than or equal to 12 for the data table to be released
without additional masking of the data. Any score over 12 will require the use of
statistical masking methods described in section 4.4 or documentation regarding the
specific characteristics of the data set that mitigate the risk.
When identifying the score for each variable, use the highest scoring criteria. For
example if a table had age groups of 0 to 11 years, 12 to 14 years, and 15 to 18 years
then the score for the “age range” variable would be +5 because the smallest age range
is 12 to 14, which is an age range of three years.
If a variable has greater granularity than the score listed, use the highest score listed.
For example, if the variable “Time” has a frequency of “weekly” then the score would be
+5 which is the maximum score associated with the most granular level (monthly) of the
variable in the Publication Scoring Criteria.
In addition to assessing the granularity of each variable, the interaction of the variables
is also important. As discussed later in section 6.4, decreasing the granularity or the
number of variables are both techniques for increasing the values for the numerators.
The final criteria in Figure 6 is that for Variable Interactions. This provides for a
subtraction of points if the only variables presented are the events (numerator), time
and geography and an addition of points for including more variables in a given
presentation. With respect to the subtraction of points, the score is based on the
minimum value for the Events variable. For example, if the smallest value for the
Events is 5 or more, then the score would be -5. However, if the smallest value for the
Events is 2, then the score would be 0. This is discussed in more detail in Section 6.2.
In assessing risk, the scoring can be part of the justification to release or not release
data but should not by itself be an absolute gateway to the release data. The review
must take into account additional considerations including those that are discussed in
this document in addition to the scoring.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 18 of 68
Figure 6: Publication Scoring Criteria
Variable
Characteristics
Score
Events (Numerator)
1000+ events in a specified population
+2
100-999 events
+3
11-99 events
+5
<11 events
+7
Sex
Male or Female
+1
Age Range
>10-year age range
+2
6-10 year age range
+3
3-5 year age range
+5
1-2 year age range
+7
Race Group
White, Asian, Black or African American
+2
White, Asian, Black or African American, American Indian or Alaska Native,
Native Hawaiian or Other Pacific Islander, Mixed
+3
Detailed Race
+4
Ethnicity
Hispanic or Latino - yes or no
+2
Detailed ethnicity
+4
Race/Ethnicity Combined
This applies when race and ethnicity are collected in a single data field
White, Asian, Black or African American, Hispanic or Latino
+2
White, Asian, Black or African American, Hispanic or Latino, American Indian
or Alaska Native, Native Hawaiian or Other Pacific Islander, Mixed
+3
Detailed Race/Ethnicity
+4
Language Spoken
English, Spanish, Other Language
+2
Detailed Language
+4
Time – Reporting Period
5 years aggregated
-5
2-4 years aggregated
-3
1 year (e.g., 2001)
0
Bi-Annual
+3
Quarterly
+4
Monthly
+5
Residence Geography*
State or geography with population >2,000,000
-5
Population 1,000,001 - 2,000,000
-3
Population 560,001 - 1,000,000
-1
Population 250,000 - 560,000
0
Population 100,000 - 250,000
+1
Population 50,001 - 100,000
+3
Population 20,001 - 50,000
+4
Population ≤ 20,000
+5
Service Geography*
State or geography with population >2,000,000
-5
Population 1,000,001 - 2,000,000
-4
Population 560,001 - 1,000,000
-3
Population 250,000 - 560,000
-1
Population of reporting region 20,001 - 250,000
0
Population of reporting region ≤20,000
+1
Address (Street and ZIP)
+3
Variable Interactions
Only Events (minimum of 5), Time, and Geography (Residence or Service)
-5
Only Events (minimum of 3), Time, and Geography (Residence or Service)
-3
Only Events (no minimum), Time, and Geography (Residence or Service)
0
Events, Time, and Geography (Residence or Service) + 1 variable
+1
Events, Time, and Geography (Residence or Service) + 2 variable
+2
Events, Time, and Geography (Residence or Service) + 3 variable
+4
* If the geography of the reporting is based on the residence of the individual, use the “Residence Geography”. If the
geography of the reporting is based on the location of service, use the “Service Geography”.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 19 of 68
4.4 Statistical Masking
If Step 3 determined that the data set has a risk that small numerators or small
denominators may result in conditions that put individuals at risk of being re-identified,
then the data set must be assessed to determine the need for statistical masking of
those small values and complimentary values. In performing the statistical masking, the
data producer must consider what level of analysis may be sacrificed in order to
produce a table with lower risk. Initial considerations for statistical masking are
described below. For additional methods related to statistical masking, please see
Section 6.4.
Reduce Table Dimensions
If there are more dimensions present in the table than necessary for the vast majority of
analysis, the data producer should consider reducing the number of dimensions in a
single table and produce multiple tables each with a subset of the dimensions in the
table that resulted in small cells. For example, if there are six dimensions of interest for
study, but a table that crosses all six dimensions produces a large number of small
cells, the data producer could consider producing several tables each of which crosses
four dimensions. This is especially effective if there are very few analytic questions
requiring a cross section of all six variables.
Reduce Granularity of Variable(s), aka Recoding or Aggregation
An alternative approach to addressing small cells in a table is to reduce the number of
levels of a particular dimension. This is especially useful for dimensions with a large
number of levels that can be easily aggregated to fewer levels and maintain much of
their utility. Geographic variables such as state or county can often be recoded into
regional variables that still serve the analytic needs of the data user. It is also the only
table restructuring option for tables with only two or three dimensions which have limited
opportunities for table dimension reduction.
It should be noted that these actions can be used alone or in tandem to reduce, or
completely eliminate, small cells within a table.
Cell Suppression and Complementary Cell Suppression
There will be cases where not all small cells can be eliminated by reducing granularity
of dimensions or the number of dimensions present in a table. In these cases it will be
necessary to suppress small cells and perform complementary suppression to ensure
that precise values of small cells cannot be calculated using the values of unsuppressed
cells and marginal values. In the simplest case this means ensuring that each column
and row of a two dimensional table has at least two suppressions. This ensures that the

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 20 of 68
precise values of the suppressed cells cannot be calculated. Complementary
suppressions are often selected using one of the methods listed below.
1. The ‘analytically least interesting’ level of a particular dimension. This is often,
‘other’, or ‘I don’t know’.
2. The smallest cell available for complementary suppression. This is based on
minimizing the ‘information loss’.
3. The cell most similar to the cell needing complementary suppression, such as
adjacent age groups. This can produce complementary suppression that may be
easier to interpret.
4.5 Legal Review
Necessity of criteria for this step will be determined by each department. This may
vary depending on the purpose of the release and whether or not the department or
program is a HIPAA covered entity or not. See Section 7 for further discussion.
4.6 Departmental Release Procedure for De-identified Data
After completion of the statistical de-identification process, each department will
specify the additional review steps necessary for public release of various data
products. Products may include but are not limited to reports, presentation, tables,
PRA responses, media responses and legislative responses. See Section 7 for
further discussion.
CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 21 of 68
5) Types of Reporting
CHHS programs develop a wide range of information based on different types of data.
This is reflected in the various categories shown on the entry page for the CHHS Open
Data Portal, which include:
Diseases and Conditions
Facilities and Services
Healthcare
Workforce
Environmental
Demographics
Resources
Various types of reporting may or may not have a connection to personal characteristics
that would create potential risk of identifying individuals.
5.1 Variables
The following list of variables is important to consider when preparing data for release.
Personal characteristics
Event characteristics
Age
Number of events
Sex
Location of event
Race
Time period of event
Ethnicity
Provider of event
Language Spoken
Location of Residence
Education Status
Financial Status
As stated previously, variables that are personal characteristics may be used to
determine a person’s identity or attributes. When these characteristics are used to
confirm the identity of an individual in a publicly released data set, then a disclosure of
an individual’s information has occurred. Individual uniqueness in the released data
and in the population is a quality that helps distinguish one person from another and is
directly related to re-identification of individuals in aggregate data. Disclosure risk is a
concern when released data reveal characteristics that are unique in both the released
data and in the underlying population. The risk of re-identifying an individual or group of
individuals increases when unique or rare characteristics are “highly visible”, or
otherwise available without any special or privileged knowledge. Unique or rare
personal characteristics (e.g., height above 7 feet) or information that isolate individuals
to small demographic subgroups (e.g., American Indian Tribal membership) increase

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 22 of 68
the likelihood that someone can correctly attribute information in the released data to an
individual or group of individuals.
Variables that are event characteristics are often associated with publicly available
information.
Therefore, increased risk occurs when personal characteristics are combined with
enough granularity with event characteristics. One could argue that if no more than two
personal characteristics are combined with event characteristics then the risk will be low
independent of the granularity of the variables. This hypothesis will need to be tested
using various population frequencies to quantify the uniqueness of the combination of
variables both the in the potential data to be released as well as in the underlying
population.
5.2 Survey Data
Survey data, often collected for research purposes, are collected differently than
administrative data and these differences should be considered in decisions about
security, confidentiality and data release.
Administrative data sources (non-survey data) such as: vital statistics (e.g. births and
deaths), healthcare administrative data (e.g. Medi-Cal utilization; hospital discharges),
reportable disease surveillance data (e.g. measles cases) contain data for all persons in
the population with the specific characteristic or other data elements of interest. Most of
the discussions in this document pertain to these types of data.
On the other hand, surveys (e.g. the California Health Interview Study) are designed to
take a sample of the population, and collect data on characteristics of persons in the
sample, with the intent of generalizing to gain knowledge suggestive of the whole
population.
The sampling methodology developed for any given survey is generally developed to
maximize the sample size with the available resources while making the sample as un-
biased (representative) as possible. These sampling procedures that are a fundamental
part of surveys generally change the key considerations for protection of security and
confidentiality. In particular, the main “population denominator” for strict confidentially
considerations remains the whole target population, not the sampled population. But, if
persons have special or external knowledge of the sampled populations (e.g. that a
family member participated in the survey), further considerations may be required.
Also, it is in the context of surveys that issues of statistical reliability often arise—which
are distinct from confidentially issues, but often arise in related discussions.
Of particular note, small numbers (e.g. less than 11) of individuals reported in surveys
do not generally lead to the same security/confidentiality concern as in population-wide

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 23 of 68
data, and as such should be treated differently than is described within the Publication
Scoring Criteria and elsewhere. In this case a level of de-identification occurs based on
the sampling methodology itself.
5.3 Budgets and Fiscal Estimates
Budget reporting may include both actuals and projected amounts. Projected amounts,
although developed with models that are based on the historical actuals, reflect
activities that have not yet occurred and, therefore, do not require an assessment for
de-identification. Actual amounts do need to be assessed for de-identification. When
the budgets reflect caseloads, but do not include personal characteristics of the
individuals in the caseloads, then the budgets are reflecting data in the Providers and
Health and Service Utilization Data circles of the Figure 2 Venn Diagram and do not
need further assessment. However, if the actual amounts report caseloads based on
personal characteristics, such as age, sex, race or ethnicity, then the budget reporting
needs to be assessed for de-identification.
5.4 Facilities, Service Locations and Providers
Many CHHS programs oversee, license, accredit or certify various businesses,
providers, facilities and service locations. As such, the programs report on various
metrics, including characteristics of the entity and the services provided by the entity.
Characteristics of the entity are typically public information, such as location, type of
service provided, type of license and the license status.
Services provided by the entity will typically need to be assessed to see if the
reporting includes personal characteristics about the individuals receiving the
services. Several examples are shown below.
a) Reporting number of cases of mental illness treated by each facility – if the
facility is a general acute care facility then the reporting of the number of cases
does not tell you about the individuals receiving the services.
b) Reporting number of cases of mental illness treated by each facility – if the
facility is a children’s hospital then the reporting of the number of cases does tell
you about the individuals receiving the services.
c) Reporting number of psychotropic medications prescribed by a general
psychiatrist does not tell you about the patients receiving the medications.
d) Reporting number of psychotropic medications prescribed by a general
psychiatrist to include the number of medications prescribed by the age group,
sex or race/ethnicity of the patients receiving the medications does tell you about
the patients receiving the medications.
In (a) and (c) above, assessment for de-identification is not necessary as there are
no characteristics about the individuals receiving the services. However, in (b) and
(d) above, the inclusion of personal characteristics which may be quasi-identifiers,

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 24 of 68
especially when combined with the geographical information about the provider,
does require an assessment for de-identification.
5.5 Mandated Reporting
CHHS programs are required to provide public reporting based on federal and California
statute and regulations, court orders, and stipulated judgments, as well as by various
funders. Although reporting may be mandated, unless the law expressly requires
reporting of personal characteristics, publicly reported data must still be de-identified to
protect against the release of identifying or personal information which may violate
federal or state law.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 25 of 68
6) Justification of Thresholds Identified
6.1 Establishing Minimum Numerator and Denominator
The DDG workgroup reviewed the published literature including information from
other states and from the federal government. There was a great deal of variation in
the numerical values chosen for the Numerator Condition. While the Centers for
Disease Control and Prevention (CDC) WONDER database suppresses cells with
numerators less than 10, the National Environmental Public Health Tracking
Network suppresses cells that are greater than 0 but less than 6. Examples range
from 3 to 40 with many being 10 to 15. The Centers for Medicare and Medicaid
Services (CMS) uses a small cell policy of suppressing values derived from fewer
than 11 individuals. As stated in a 2014 publication associated with a data release
of Medicare Provider Data, “to protect the privacy of Medicare beneficiaries, any
aggregated records which are derived from 10 or fewer beneficiaries are excluded
from the Physician and Other Supplier PUF [public use file].”
11
Of note, CMS only
uses a Numerator Condition.
Just as there is no consistent value for the Numerator Condition, neither is there a
consistent value for the Denominator Condition. Some examples include:
National Center for Health Statistics (public micro-data) – 250,000
National Environmental Health Tracking Network – 100,000
Maine Integrated Youth Health Survey – 5,000
In establishing a minimum denominator to protect confidentiality, the DDG
workgroup began by looking at the risk associated with providing geography
associated with record level data. As noted in the “Guidance Regarding Methods for
De-identification of Protected HIPAA Privacy Rule”, published November, 2012 by
the U.S. Department of Health & Human Services, Office for Civil Rights there is
varying risk based on the level of zip code and how the zip code is combined with
other variables. It has been estimated that the combination of a patient’s Date of
Birth, Sex, and 5-Digit ZIP Code is unique for over 50% of residents in the United
States.
12
,
13
This means that over half of U.S. residents could be uniquely described
just with these three data elements. In contrast, it has been estimated that the
11
“Medicare Fee-For Service Provider Utilization & Payment Data Physician and Other Supplier Public
Use File: A Methodological Overview,” Prepared by: The Centers for Medicare and Medicaid Services,
Office of Information Products and Data Analytics, April 7, 2014.
12
See P. Golle. Revisiting the uniqueness of simple demographics in the US population. In Proceedings
of the 5th ACM Workshop on Privacy in the Electronic Society. ACM Press, New York, NY. 2006: 77-80.
13
See L. Sweeney. K-anonymity: a model for protecting privacy. International Journal of Uncertainty,
Fuzziness, and Knowledge-Based Systems. 2002; 10(5): 557-570.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 26 of 68
combination of Year of Birth, Sex, and 3-Digit ZIP Code is unique for approximately
0.04% of residents in the United States.
14
For this reason, the HIPAA Safe Harbor
rule specifies that the 3-Digit ZIP Code can be provided at the record level if the 3-
Digit ZIP Code has a minimum of 20,000 people. By aggregating data for a given 3-
Digit ZIP Code, the potential for identifying a unique individual is less than 0.04%.
By combining with the Numerator Condition, the risk becomes less than 0.04%
because there will be a minimum of 11 individuals with a particular age and sex for
the 3-Digit ZIP Code. Additionally, most tables will provide additional levels of
aggregation further reducing risk. This reduction of risk is discussed further with
respect to the Publication Scoring Criteria.
A minimum denominator of 20,000 was chosen as part of the numerator-
denominator condition to leverage the risk assessment cited above.
The Numerator-Denominator Condition serves as an initial screening to assess
potential risk for a data set. If this condition is met, additional analysis is not
necessary. If the condition is not met, then the analysis proceeds to Step 3.
6.2 Assessing Potential Risk – Publication Scoring Criteria
The Publication Scoring Criteria is provided as an example of a method that meets
the requirements of Step 3 in the Data Assessment for Public Release Procedure. It
is a tool to assess and quantify potential risk for re-identification of de-identified data
based on two identification risks: size of potential population and variable specificity.
The Publication Scoring Criteria is used to assess the need to suppress small cells
as a result of a small numerator, small denominator, or both small numerator and
small denominator where a small numerator is less than 11 and a small denominator
is less than 20,001. That is why the Publication Scoring Criteria takes into account
both numerator (e.g., Events) and denominator (e.g., Geography) variables.
The Publication Scoring Criteria is based on a framework that has been in use by
the Illinois Department of Public Health, Illinois Center for Health Statistics. Various
other methods have been used to assess risk and the presence of sensitive or small
cells. Public health has a long history of public provision of data and many methods
have been used. Further discussion of other methods used to assess tables for
sensitive or small cells is found in Section 6.3.
This section provides a more detailed review of the criteria that make up the
Publication Scoring Criteria.
14
See L. Sweeney. Testimony before that National Center for Vital and Health Statistics Workgroup for
Secondary Uses of Health information. August 23, 2007.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 27 of 68
Events
Variable
Characteristics
Score
Events
1000+ events in a specified population
+2
100-999 events
+3
11-99 events
+5
<11 events
+7
The Events score represents a score for the numerator. The Events category will be
scored based on the smallest cell size in the table.
The lowest value for the Events variable (<11 events) which has the highest score
(+7) was chosen to be consistent with the Numerator Condition. The Publication
Scoring Criteria is used when the Numerator-Denominator Condition is not met.
Therefore, when the Numerator Condition is not met with respect to the Events
variable, a high score is given.
Sex
Variable
Characteristics
Score
Sex
Male or Female
+1
Sex is commonly represented as two categories: male and female. Because the
number of categories is small, just knowing a person’s reported sex is not enough to
pose a risk of identifying that person. The score of +1 reflects that inclusion of the
variable in a table introduces increased specificity; however, that it only has two
potential values gives it a low risk.
In cases where an additional stratification of other/unknown is used for sex, the
reviewer will need to assess potential for increased risk based on the inclusion of the
additional stratification.
Although the variable “Sex” is often called “Gender”, it should not be confused with
the variables “sexual orientation” and “gender identity.” According to definitions from
the American Psychological Association, “Sexual orientation refers to the sex of
those to whom one is sexually and romantically attracted” and “Gender identity
refers to “one’s sense of oneself as male, female, or transgender.”
15
15
Definition of Terms: Sex, Gender, Gender Identity, Sexual Orientation; Excerpt from: The Guidelines for
Psychological Practice with Lesbian, Gay, and Bisexual Clients, adopted by the APA Council of
Representatives, February 18-20, 2011. http://www.apa.org/pi/lgbt/resources/sexuality-definitions.pdf

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 28 of 68
Additional information is provided from San Francisco County at
https://www.sfdph.org/dph/files/hc/HCFinance/agendas/2014/August%205/pdf%20re
v%20072514%20re%20age%20adopted%20090313%20-
%20SFDPH%20Sex%20and%20Gender%20Guidelines.pdf.
Age Range
Variable
Characteristics
Score
Age Range
>10-year age range
+2
6-10 year age range
+3
3-5 year age range
+5
1-2 year age range
+7
Age ranges receive a higher score for smaller ranges of years due to the increased
risk for identification.
Of note, the HIPAA Safe Harbor method specifically identifies the following as an
identifier: “All elements of dates (except year) for dates that are directly related to an
individual, including birth date, admission date, discharge date, death date, and all
ages over 89 and all elements of dates (including year) indicative of such age,
except that such ages and elements may be aggregated into a single category of
age 90 or older.” Although dates are included in the Safe Harbor list, age (<90 years
old) is not. The risk score to age ranges reflects the two components of the scoring
criteria: size of the potential population and the variable specificity.
Race Group and Ethnicity
Race Group
White, Asian, Black or African American
+2
White, Asian, Black or African American,
American Indian or Alaska Native, Native
Hawaiian or Other Pacific Islander, Mixed
+3
Detailed Race
+4
Ethnicity
Hispanic or Latino - yes or no
+2
Detailed ethnicity
+4
Race/Ethnicity
Combined
This applies when race and ethnicity are
collected in a single data field
White, Asian, Black or African American,
Hispanic or Latino
+2
White, Asian, Black or African American,
Hispanic or Latino, American Indian or Alaska
Native, Native Hawaiian or Other Pacific
Islander, Mixed
+3
Detailed Race/Ethnicity
+4

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 29 of 68
Race and Ethnicity are collected in a number of different ways on the different state
and federal data collection tools. At the federal level, starting in 1997, Office of
Management and Budget required federal agencies to use a minimum of five race
categories:
White,
Black or African American,
American Indian or Alaska Native,
Asian, and
Native Hawaiian or Other Pacific Islander.
Ethnicity asks individuals if they are Hispanic or Latino. Additional specificity for
Ethnicity may be requested.
The California population in general is approximately:
16
40% White
13% Asian
6% Black or African American
<1% American Indian
<1% Native Hawaiian and other Pacific Islander
37% Hispanic or Latino
Based on these percentages, Race Group at the level of White, Asian and Black or
African American is given a score of +2 because the Asian and Black or African
American groups are relatively small. If the reporting is for the OMB standard
categories, White, Asian, Black or African American, American Indian or Alaska Native,
Native Hawaiian or Other Pacific Islander, and Mixed, then the score is +3. If more
specificity is requested for Race Groups the score is +4 because the other groups
are much smaller at less than 1% of the overall population. Similarly, for the
Hispanic or Latino Ethnicity the score is a +2 for a yes or no answer, whereas more
detailed ethnicity results in a higher score of +4.
For Race/Ethnicity Combined fields, the scoring is +2 for the groups White, Asian,
Black or African American, Hispanic or Latino. The score is +3 for the OMB standard
categories with Hispanic or Latino, White, Asian, Black or African American, American
Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, and Mixed. The
score is +4 for more detailed categories.
16
Based on Year 2010 from the State of California, Department of Finance, Report P-1 (Race): State and
County Population Projections by Race/Ethnicity, 2010-2060. Sacramento, California, January 2013

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 30 of 68
Race and Ethnicity demographics may vary significantly based on geography as well
as based on particular conditions. So although the scoring criteria presents a
guideline for assessing risk, the population frequencies for the specific geography
and/or condition should also be taken into account. Appendix C provides the county
specific demographics produced by Department of Finance for reference.
Three scenarios are presented to help demonstrate how to use the three race group
and ethnicity scoring criteria.
First Scenario – Complete Cross-Tabulation between Race and Ethnicity
Consider this table:
Hispanic
Non-Hispanic
Black
50
250
300
White
200
1000
1200
Asian
5
95
100
255
1345
1600
This is the most granular you can get, so you would add both the Race and Ethnicity
score to the overall total for your scoring metric (i.e. greatest risk for re-
identification). Note that you can replace “Ethnicity” with “Sex” and the principle still
applies—you have a cross-tabulated table of Race and Sex.
Second Scenario – Race and Ethnicity merged into exclusive categories
Usually the algorithm is that Ethnicity trumps Race when categorizing. This results in
a Hispanic category, with the other categories effectively becoming “Non-Hispanic
Race.” So the above table would become:
Black 250
White 1000
Asian 95
Hispanic 255
This is when you would use the combined Race/Ethnicity score in the guidelines for
your scoring metric.
Third Scenario – No Interaction between Race and Ethnicity
If you did this, the above table would become:
Black 300
White 1200
Asian 100

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 31 of 68
Hispanic 255
Note that this is the only scenario where you can’t add up all the categories to get a
total population. Also you would need to run the scoring metric separately for your
Race-only and Ethnicity-only datasets. Like the First Scenario, you can replace
Ethnicity with Sex and it still makes sense—you now have two tables, one displaying
Race and the other Sex, with no interaction between the two—which lessens the
Small Cell Size problem.
Language Spoken
Variable
Characteristics
Score
Language Spoken
English, Spanish, Other Language
+2
Detailed Language
+4
Language spoken is captured in a variety of data systems to support individuals in
receiving services in the language they speak. The following table is taken from the
report: Medi-Cal Beneficiaries by Primary Language Report of October, 2010.
17
This
frequency distribution was used to determine the groupings for the scoring above.
Language Spoken
Count of Medi-
Cal Members
Percent of Count
Total
7,835,022
100.00
English
4,135,060
52.78
Spanish
2,840,758
36.26
Vietnamese
141,289
1.80
Cantonese
85,750
1.09
Armenian
65,096
0.83
Russian
41,252
0.53
Tagalog
39,361
0.50
Mandarin
35,330
0.45
Hmong
33,594
0.43
Korean
27,814
0.35
Farsi
26,123
0.33
Arabic
23,929
0.31
Cambodian
20,476
0.26
Lao
8,355
0.11
Other Chinese
7,483
0.10
Mien
3,803
0.05
Sign Language
2,637
0.03
Thai
1,940
0.02
Portuguese
1,666
0.02
Ilocano
1,661
0.02
17
http://www.dhcs.ca.gov/services/MH/InfoNotices-Ltrs/Documents/InfoNotice-PrimaryLang-
Enclosure1.pdf

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 32 of 68
Language Spoken
Count of Medi-
Cal Members
Percent of Count
Samoan
1,306
0.02
Japanese
1,215
0.02
French
653
0.01
Turkish
376
0.00
Hebrew
367
0.00
Polish
275
0.00
Italian
252
0.00
Other and unspecified
287,201
3.67
Based on the above numbers, the majority of individuals speak English or Spanish.
Therefore if the table includes “English”, “Spanish”, and “Other Language” as the
categories for “Language Spoken”, then the score is +2 which is comparable to
reporting Hispanic or Latino Ethnicity as a “Yes or No”.
As noted for Race and Ethnicity demographics, language spoken demographics may
vary significantly based on geography as well as based on particular conditions. So
although the scoring criteria presents a guideline for assessing risk, the population
frequencies for the specific geography and/or condition should also be taken into
account.
If more specificity for Language Spoken is being requested with respect to reporting
on the other languages in the table above, the request will need to be reviewed on a
case by case basis. The additional review is necessary given the variability of
language spoken by different populations or geographies and the consideration for
potential increased risk of identification.
Time – Reporting Period
Variable
Characteristics
Score
Time – Reporting Period
5 years aggregated
-5
2-4 years aggregated
-3
1 year (e.g., 2001)
0
Bi-Annual
+3
Quarterly
+4
Monthly
+5
Many reports are published based on the calendar year. However, the combination
of years of data is an excellent way to provide increased aggregation in a way that
allows for more specificity elsewhere, such as county identifiers. Inversely, the
smaller the time period in the data, the closer the time period comes to
approximating a date. Thus monthly reported data has a high score of +5.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 33 of 68
Of note, the HIPAA Safe Harbor method list includes “All elements of dates (except
year) for dates that are directly related to an individual, including birth date,
admission date, discharge date, death date, and all ages over 89 and all elements of
dates (including year) indicative of such age, except that such ages and elements
may be aggregated into a single category of age 90 or older.” This is a potential
identifier when in combination with other information. This potential as an identifier
influences the higher scores in the Publication Scoring Criteria as the time period for
aggregation gets smaller.
The “0” value for this variable is set at one year as this is the criteria for Safe Harbor
under the HIPAA de-identification standard.
Geography
Variable
Characteristics
Score
Residence Geography*
State or geography with population >2,000,000
-5
Population 1,000,001 - 2,000,000
-3
Population 560,001 - 1,000,000
-1
Population 250,000 - 560,000
0
Population 100,000 - 250,000
+1
Population 50,001 - 100,000
+3
Population 20,001 - 50,000
+4
Population ≤ 20,000
+5
Service Geography*
State or geography with population >2,000,000
-5
Population 1,000,001 - 2,000,000
-4
Population 560,001 - 1,000,000
-3
Population 250,000 - 560,000
-1
Population of reporting region 20,001 - 250,000
0
Population of reporting region ≤20,000
+1
Address (Street and ZIP)
+3
* If the geography of the reporting is based on the residence of the individual, use the
“Residence Geography”. If the geography of the reporting is based on the location of
service, use the “Service Geography”.
The Geography score, while it may or may not represent the denominator of the
table, does provide a reference to the base population about which the reporting is
occurring. This will often be reflected in the title of the table if a statewide table.
Otherwise the geography may be represented in the rows or columns. There are
two different scoring sets based on whether the geography reporting is based on the
residence of the individual to which the information applies or to the service location.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 34 of 68
The scores are higher for geography related to residence address because so much
information is publicly available about individuals and their address of residence.
For large populations greater than 560,000, which is equivalent to the size of a state,
there is a negative score because the size of the denominator masks the individual.
The number 560,000 was chosen as a cut-off because this is the size of the smallest
state (Wyoming). We chose to use the cut-off at the smallest state’s population
because state level reporting is not listed as one of the 18 identifiers the HIPAA Safe
Harbor method.
The scores for the service geography are lower because clients can generally come
from diverse locations for services. Although people often seek services or have
health conditions close to their homes, they may also travel extensive distances.
Reviewers do need to make sure that there are not constraints associated with
services that would mean the service geography and resident geography are the
same. For example, if a program publishes service utilization by county and the
county services can only be used by county residents, then the service utilization by
county is also the county of residence. Scoring should be based on the criteria that
results in the highest score and thus the highest risk.
Service Geography includes a level of detail that is identified as “Address (Street
and ZIP).” This deals with reporting by provider (hospital, clinic, provider office, etc.)
Provider addresses are public information and are public at the street address level.
A given provider will tend to have a standard catchment area or the geographic
boundaries from which most patients come from. This information is published by
Office of Statewide Health Planning and Development (OSHPD)
18
for hospitals.
While this addresses where most patients or clients come from, patients or clients
may also come from outside the catchment area. For that reason this does not
score as high as the more detailed geography under Residence Geography.
Variable Interactions
Variable
Characteristics
Score
Variable Interactions
Only Events (minimum of 5), Time, and Geography
(Residence or Service)
-5
Only Events (minimum of 3), Time, and Geography
(Residence or Service)
-3
Only Events (no minimum), Time, and Geography
(Residence or Service)
0
18
Office of Statewide Health Planning and Development (OSHPD), Patient Origin & Market Share
Reports, Retrieved from
http://www.oshpd.ca.gov/HID/Products/PatDischargeData/PivotTables/PatOrginMkt/default.asp on
January 22, 2016.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 35 of 68
Events, Time, and Geography (Residence or
Service) + 1 variable
+1
Events, Time, and Geography (Residence or
Service) + 2 variables
+2
Events, Time, and Geography (Residence or
Service) + 3 variables
+4
This criteria specifically addresses the interaction of the variables in a given data
presentation and requires the analyst to identify dependent as opposed to
independent variables. This criteria is used with respect to dependent variables.
This is demonstrated in the two tables below.
Illustration A: Dependent Variables
In this example the Event (counts of Disease A) is shown for Males who are also 0-
17 years old or Males who are also 18-25 years old. In this case Sex and Age are
dependent because the stratification for each variable is stacked. This commonly
occurs in pivot tables.
Counts of
disease A by
year
Males and
0-17 years old
Males and
18-25 years old
Females and
0-17 years old
Females and
18-25 years
old
Year 1
6
10
5
8
Year 2
8
14
3
20
Illustration B: Independent Variables
In this example the Event (counts of Disease A) is for Males or Females which is
shown side by side to a table with ages 0-17 years old or 18-25 years old. In this
case Sex and Age are independent because the stratification for each variable is not
stacked. Although the two variables Sex and Age are shown in the same table, they
are presented independently of each other. While you can compile the data in
Example B from Example A, the reverse is not true.
Counts of
disease A by
year
Males
Females
0-17 years old
18-25 years
old
Year 1
16
13
11
18
Year 2
22
23
11
34

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 36 of 68
This criteria is structured to have less impact if personal characteristics outside of
time and geography are excluded and more impact if multiple personal
characteristics are included. This provides for a subtraction of points if the only
variables presented are the events (numerator), time and geography and an addition
of points for including more variables in a given presentation. With respect to the
subtraction of points, the score is based on the minimum value for the Events
variable. For example, if the smallest value for the Events is 5 or more, then the
score would be -5. However, if the smallest value for the Events is 2, then the score
would be 0.
The minimum value for Events of 3 (Only Events (minimum of 3), Time, and
Geography (Residence or Service)) is used as a threshold to address concern for
pre-existing knowledge by users about individuals. For example, if an entity knows
who one person is with disease A and the count for Events is “1” or “2”, then the
entity could identify the person they know of or the person they know of plus
information about the other person. The use of a minimum of 3 does not protect
against two entities colluding to determine a third person.
19
For this reason, the
threshold of 5 for Events is also given. The threshold of 5 is frequently used in
public health reporting regarding various events.
In contrast, if additional demographic variables are added, then the risk increases
significantly. For example, for Events, Time and Geography (Residence or Service)
with three additional variables, a table would show how many individuals are female
by age group by race for a given time period and geography. This allows for a more
detailed comparison to census data and assessment of the number of individuals
with a particular set of characteristics.
20
For this reason, additional points are added
because of the inclusion of multiple dependent variables.
Other Variables
Variables other than those specified in the Publication Scoring Criteria can be
released only after an additional review by the department’s Statistical Expert on a
case by case basis. A guideline that can be considered in performing this review is
the following scoring.
19
NORC, “NORC Recommendations for California Department of Health Care Services (DHCS) Data De-
Identification Guidelines (DDG),” January 8, 2016.
20
NORC, “Case Study: The Disclosure Risk Implications of Small Cells Combined with Multiple Tables or
External Data,” January 8, 2016.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 37 of 68
Variable
Characteristics
Score
Other Variables
<5 groups or categories
+3
5-9 groups
+5
10+ groups
+7
Considerations include not just the number of groups, but also the characteristics of
the variables. Consider whether the variable represents an aggregation (Diagnosis
Related Groups) or a specific item (ICD-10 Code). Also consider the availability of
the variable to the public when also associated with other information, in particular
with variables that may be personal characteristics.
6.3 Assessing Potential Risk – Alternate Methods
As noted in Section 6.2, the Publication Scoring Criteria is based on a framework
that has been in use by the Illinois Department of Public Health, Illinois Center for
Health Statistics. Various other methods have been used to assess risk and the
presence of sensitive or small cells. Public health has a long history of public
provision of data and many methods have been used. Some of those methods are
highlighted here.
Ohio Department of Health published a Data Methodology Standards for
Public Health Practice.
21
This method is framed around the concept that a
Disclosure Limitation Standard for tabulations of confidential Ohio Department
of Health data shall be suppressed when the table denominator value minus
the table numerator value is less than 10.
Washington State Department of Health published Guidelines for Working
with Small Numbers
22
that highlights many topics covered in the CHHS DDG
but also discusses the use of relative standard error (RSE) to assess
reliability of data in addition to steps to take protect confidentiality.
Colorado Department of Public Health and Environment published Guidelines
for Working with Small Numbers
23
which also addresses many of the same
topics.
The size of numerators and denominators vary in each of the documents above
although the principles are consistent.
21
Ohio Department of Public Health. “Data Methodology for Public Health Practice.”
http://www.odh.ohio.gov/~/media/ODH/ASSETS/Files/data%20statistics/standards/methodological%20sta
ndards/disclimit.ashx.
22
Washington State Department of Health. "Guidelines for Working with Small Numbers." N.p., 15
October 2012. Retrieved from http://www.doh.wa.gov/Portals/1/Documents/5500/SmallNumbers.pdf.
23
Colorado Department of Public Health and Environment. “Guidelines for Working with Small Numbers.”
Retrieved from http://www.cohid.dphe.state.co.us/smnumguidelines.html

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 38 of 68
6.4 Statistical Masking
Statistical masking provides an extensive set of tools that can be used to mitigate
potential risk in a given data presentation. As discussed in Section 4.4, the data
releaser will assess the need for statistical masking when the assessment in Step 3
identified potential risk. Each department will document statistical masking
processes that are routinely used in data preparation for public release.
As discussed in section 4.4, initial methods to address sensitive or small cells, as
well as complimentary cells include the following:
Reduce Table Dimensions
Reduce Granularity of Variable(s), aka Recoding or Aggregation
Cell Suppression and Complementary Cell Suppression
Small cell sizes are typically encountered when one of the following conditions is
met.
a) Multiple variables. This most often occurs in a pivot table presentation or a
query interface where a user may have occurrences of disease X, stratified by
county, stratified by sex, stratified by race and ethnicity.
b) Granular variables. The more granular the variable the smaller the potential
numerator and denominator. This most commonly occurs with shortening the
time period of reporting (weekly) or making the geography more specific (zip
code or census tract). However, it can also occur when there are many
categories for a variable. An example of this is aid codes in Medi-Cal where
there are almost 200 aid codes.
c) Rare events. Examples include diseases such as hemophilia. Examples of
incidents may result from mass trauma events such as a plane crash or multi-
car accident.
In each of these cases, statistical masking may be addressed in a number of ways.
For this reason, it is important to keep in mind the purpose for the reporting so that
the method chosen for masking can still maximize the usefulness of the data
provided. Choices for each condition are highlighted below.
a) Multiple variables. Options include separating the table into multiple tables
that limit the number of variables included in each table; decreasing the
granularity of the variables included in the table; or suppressing the small cell
with an indicator that it is less than 11.
b) Granular variables. A common approach to this situation would be to
decrease the granularity of the variables although suppressing the small cell
with an indicator that it is less than 11 is also an option.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 39 of 68
c) Rare events. In these cases it becomes very challenging to suppress the
value in a way that it will not be able to be used with other public information
to identify individuals. Additionally, with rare events, there is more
significance in the variance of small numbers.
In addition to small cells, complementary cells must also be suppressed.
Complementary cells are those which must be suppressed to prevent someone from
being able to calculate the suppressed cell based on row or column totals in
combination with other data in that row or column.
Suppressing small cell values and complimentary cells can be done in two ways.
1) Use a symbol to indicate the cell has been suppressed. Identify any other
cells (complimentary cells) that can be used to calculate the small cell and
use a symbol to indicate the cell has been suppressed.
2) Use a symbol to indicate the cell has been suppressed or leave the cell blank
and remove the value from all pertinent row and column totals so that the cell
cannot be calculated. This negates the need for evaluation of complementary
cells. This method must be used with great caution because the totals may
actually be published in other non-related tables. For this reason the method
is not recommended.
When suppressing values, the following footnote to indicate the suppression is
recommended:
“Values are not shown to protect confidentiality of the individuals summarized
in the data.”
In addition to the above, there are a number of other methods that may be used for
Statistical Masking. Methods discussed in the “Statistical Policy Working Paper 22
(Second version, 2005), Report on Statistical Disclosure Limitation Methodology”
include the following for tables of counts or frequencies and for magnitude data.
24
Tables of Counts or Frequencies
Sampling as a Statistical Disclosure Limitation Method
Defining Sensitive Cells
o Special Rules
o The Threshold Rule
Protecting Sensitive Cells After Tabulation
o Suppression
24
Federal Committee on Statistical Methodology, Statistical Policy Working Paper 22 – Report on
Statistical Disclosure Limitation Methodology. Washington: Statistical Policy Office, Office of
Management and Budget, 1994.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 40 of 68
o Random Rounding
o Controlled Rounding
o Controlled Tabular Adjustment
Protecting Sensitive Cells Before Tabulation
Tables of Magnitude Data
Defining Sensitive Cells – Linear Sensitivity Rules
Protecting Sensitive Cells After Tabulation
Protecting Sensitive Cells Before Tabulation

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 41 of 68
7) Approval Processes
After completion of the statistical de-identification process, each department will specify
the additional review steps necessary for public release. This may vary depending on
the purpose of the release and whether or not the department/program is a HIPAA
covered entity.
Recognizing that some data analyses may be published as independent tables while
other analyses will be part of larger reports, the final review of all data analyses must
follow the department or office procedures for document review in addition to review
procedures identified for the implementation of the DDG. The expectation is that the
review of data for de-identification will fit into other routine review processes. Reviews
outside the DDG portion may vary depending on whether data is being released for a
PRA request, to the media, to the legislature, by the program as part of routine
reporting, or for other reasons.
Departments and offices may consider the following components for reviews related to
data that has been de-identified.
Statistical Review to Assess De-identification
(for HIPAA entities this may be an Expert Determination Review)
Legal Review
Departmental Release Procedures
Statistical Review to Assess De-identification (Steps 1, 2, 3 & 4)
The department or office may designate individuals within the department to provide a
statistical review of data products before they are released to ensure the data has been
de-identified with methods that are consistent with these guidelines.
For HIPAA covered entities, this will be performed by individuals who are considered
experts for the purpose of performing expert determinations in compliance with the
HIPAA Privacy Rule, and who meet the Rule’s implementation specifications: “A person
with appropriate knowledge of and experience with generally accepted statistical and
scientific principles and methods for rendering information not individually identifiable”
[45 CFR Section 164.514(b)(1)] This expert determination review, according to the
regulation’s requirements, will be performed by:
“(1) A person with appropriate knowledge of and experience with generally
accepted statistical and scientific principles and methods for rendering
information not individually identifiable:
(i) Applying such principles and methods, determines that the risk is very
small that the information could be used, alone or in combination with

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 42 of 68
other reasonably available information, by an anticipated recipient to
identify an individual who is a subject of the information; and
(ii) Documents the methods and results of the analysis that justify such
determination”
25
When an expert determination review is requested, the Expert Determination Review
must include a document that includes the expert’s determination that “the risk is very
small that the information could be used, alone or in combination with other reasonably
available information, by an anticipated recipient to identify an individual who is a
subject of the information,” attests that the requirements of 45 CFR section 164.514
(b)(1)(i) and (ii) have been met, and includes (or attaches) the documentation required
by 45 CFR section 164.514(b)(1)(ii). This document must be signed by the expert.
These guidelines provide a starting point for expert determination review; however, the
facts of each case chosen for expert determination review must be analyzed on an
individual, case-by-case basis by the expert. If followed, the Guidelines may be
referenced as part of the documentation used to support the expert determination. The
documentation should also include a general description of the principles, methods, and
analyses used, as well as an explanation of the analysis that justifies the expert
determination.
The expert determination review may use the Expert Determination Template in
Appendix A. The Expert Determination Template includes a confirmation that “the risk
is very small that the information could be used, alone or in combination with other
reasonably available information, by an anticipated recipient to identify an individual
who is a subject of the information.”
If methods that have been used to de-identify the data are not described in the
Guidelines, then the Expert will need to provide additional documentation that explains
the statistical and scientific principles and methods used and the results of the
additional analysis.
Legal Review (Step 5)
Step 5 in the Data Assessment for Public Release Process provides for a legal review
within the department. This may vary depending on the purpose of the release and
whether or not the department or program is a HIPAA covered entity or not. This review
may assess the data to be released for risk to the Department, and for potential
implications on litigation, statutory or regulatory conditions on data release, and other
legal considerations that may impact release. Legal Services may review the expert
25
45 CFR section 164.514 (b)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 43 of 68
determination documentation to ensure compliance with the HIPAA Privacy Rule as
applicable.
Departmental Release Procedures (Step 6)
Step 6 in the Data Assessment for Public Release Process provides for departmental
release procedures for de-identified data. After completion of the statistical de-
identification process, each department will specify the additional review steps
necessary for public release of various data products. Products may include but are not
limited to reports, presentation, tables, PRA responses, media responses and legislative
responses.
Potential reviews include Public Affairs. Public Affairs is often designated to receive all
publications, brochures, or pamphlets intended for public distribution to be printed or
reproduced to review the material to determine if it requires Agency Approval or
Governor’s Office approval. Public Affairs may also be designated to review content to
assess the data table for compliance with the Americans with Disabilities Act of 1990
26
(ADA).
Departments may also consider processes for quality assurance reviews: The may
apply to data products being added to the web sites to ensure that they have had
appropriate reviews and de-identification steps. It may also include reviews of updated
reports. Many reports maintain the same variables and formats but have updated
numbers/information on a periodic basis (monthly, quarterly, annually). For these
reports, departments may consider a centralized review to ensure data products are
consistent with previously reviewed reports and have not had changes that would
change the previous assessment.
26
42 U.S.C 12101 et seq.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 44 of 68
8) DDG Governance
Governance for DDG will be provided by the Data Subcommittee with support from the
Risk Management Subcommittee. The Subcommittees are part of the CHHS
governance structure as described in the CHHS Information Strategic Plan.
27
Governance for the CHHS DDG will provide the following support for departments and
offices.
Maintain the CHHS DDG, which will include updates and revisions to the
document as well as annual reviews for currency.
Coordinate integration of the CHHS DDG into the Statewide Health Information
Policy Manual (SHIPM), Section 2.5.0 De-identification
28
and the CHHS Open
Data Handbook.
Convene a Peer Review Team (PRT).
Provide for escalation of issues that cannot be resolved by the PRT.
The CHHS PRT will include no more than two representatives from each department or
office. Membership of the PRT is expected to include individuals with the following
background and experience.
Knowledge of and experience with generally accepted statistical and scientific
principles and methods for rendering information not individually identifiable.
Knowledge of and experience with legal principles associated with data de-
identification in compliance with California IPA and HIPAA.
The PRT will have the following responsibilities:
Provide review and consultation regarding a department’s DDG to ensure it is
consistent with the CHHS DDG. This may be particularly useful if a department
incorporates methods for de-identification in the department’s DDG that have not
already been documented in the CHHS DDG.
Provide for escalation and review of data de-identification questions or issues
that a department is not comfortable resolving independently.
Develop training tools to be used by departments when developing and
implementing department specific DDGs based on the content of the CHHS
DDG.
The PRT will not review all disclosures or data released by each department.
27
California Health and Human Services Agency, Information Strategic Plan 2016.
28
http://www.ohi.ca.gov/calohi/ohii-shipm-manual.htm

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 45 of 68
9) Publicly Available Data
A critical step in reviewing data for public release is the consideration of what other data
may be publicly available that could be used in combination with the newly released
data to identify the individuals represented in the data. This section will highlight some
specific data sets that are publicly available that may be used in combination with
CHHS data that would contribute to potential increased risk.
Common kinds of data with personal information include: real estate records, individual
licensing databases (MD, RN, contractors, lawyers, etc.), marriage records, news (and
other) media reports, commercially available databases (data brokers, marketing), court
documents, etc.
Vital Records Data
Another common data set for programs to be aware of are the publicly available
electronic birth and death indices from Vital Records, as specified in Health and Safety
Code section 102230(b).
The following are provided in the birth record indices:
First, middle, and last name
Sex
Date of birth
Place of birth
The following are provided in the death record indices:
First, middle, and last name
Sex
Date of birth
Place of birth
Date of death
Place of death
Father’s last name
Other potential sources of publicly available data to consider are informational certified
copies of birth and death certificates. In California, anyone can obtain an informational
certified copy of birth and death certificates, which are clearly marked as un-authorized
copies that cannot be used to verify identity. In reality, it is difficult to use these as a
dataset for the following reasons:

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 46 of 68
Certified copies of birth and death certificates must be obtained on an individual
basis, and you must be able to identify the record. In other words, an individual
cannot simply ask for a stack of certificates for purposes of creating a dataset.
Certified copies are issued on specialized banknote paper, not in electronic
format, which creates a problem of scale when trying to create a dataset.
There is a $25 fee for each certified copy of a birth certificate and $21 for a
certified copy of a death certificate, which also creates a problem of scale when
trying to create a dataset.
Certified copies are meant for individual use. A request for a large amount of
certificates may generate an investigation among vital records staff as to why so
many certificates were requested at once.
CHHS Open Data Portal
As additional data sets are added to the Open Data Portal, programs need to take that
information into account when considering potential risk for any given data set. The
CHHS Open Data Workgroup will be providing easier access to both lists of data
currently on the portal as well as data sets planned for addition to the porta. While
significant with over 100 data sets, this is not exhaustive because of the PRA, which
allows for an extremely broad amount of information to be released in a sporadic way.
So some specificity can occur but not completely. CHHS departments have a duty of
due diligence in the de-identification process regarding consideration of published
identifiable data, published de-identified data and the soon to be published de-identified
data.
Listed below are individual records or documents that the Department of Rehabilitation
have available to the public:
Fair Hearing Decisions include appellant’s initials and possibly other information,
depending on issue appellant presents for hearing, such as sex, disability,
employment, education, vocational rehabilitation services, etc.; and
Monthly Operating Reports and information therefrom includes names of
licensees and financial information regarding the operation of the licensees’
operation of vending facilities in the Business Enterprises Program for the Blind.
To be eligible for this program, the individuals must be legally blind.
Public Census and Demographic Information
The Demographic Research Unit (DRU) of the California Department of Finance is
designated as the single official source of demographic data for state planning and
budgeting.
29
The DRU produces the following products which serve as the basis for
29
http://www.dof.ca.gov/research/demographic/dru/index.php

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 47 of 68
understanding the population characteristics and distributions that frequently make up
the denominators in the review of data sets.
Estimates - Official population estimates of the state, counties and cities
produced by the Demographic Research Unit for state planning and budgeting.
Projections - Forecasts of population, births and public school enrollment at the
state and county level produced by the Demographic Research Unit.
State Census Data Center - Demographic, social, economic, migration, and
housing data from the decennial censuses, the American Community Survey, the
Current Population Survey, and other special and periodic surveys.
Commonly Shared Information
With the growth of social media, people frequently share information through tools such
as Facebook, Linked In, and Tweets. While it would be impossible to take into account
all information that people make public about themselves, there is an expectation that a
certain amount of information is likely to be in the public domain based on information
individuals frequently provide about themselves. Examples of such information include
wedding dates, birth dates, education (high school, college) and professional
certifications.
Geographic Information
Geographic information is particularly suited to being combined with other geographic
information given the relatively standardized was data is coded (latitude, longitude,
county, etc.) With the use of mapping tools, various information can be combined in a
way that is called a “mash up.” “A mashup, in web development, is a web page, or web
application, that uses content from more than one source to create a single new service
displayed in a single graphical interface. For example, you could combine the
addresses and photographs of your library branches with a Google map to create a map
mashup.[1] The term implies easy, fast integration, frequently using open application
programming interfaces (open API) and data sources to produce enriched results that
were not necessarily the original reason for producing the raw source data.”
30
30
http://en.wikipedia.org/wiki/Mashup_(web_application_hybrid)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 48 of 68
10) Development Process
The CHHS Data Subcommittee requested the convening of the CHHS Data De-
Identification Workgroup to develop the DDG.
The DDG Workgroup began with an orientation to the topic of data de-identification and
presentations by the DHCS, OSHPD and California Department of Public Health
(CDPH) regarding current practices and activities related to data de-identification. The
DDG Workgroup used the Public Aggregate Reporting for DHCS Business Reports
(PAR-DBR) as a starting point for initial drafts. The PAR-DBR had been developed
between April and August, 2014 through a workgroup processes within DHCS with input
and presentations from OSHPD, CDPH, and University of California, Los Angeles
California Health Interview Survey. The PAR-DBR served as a basis for this document,
including the literature review conducted as part of the development of the PAR-DBR.
The development process was designed to include an updated literature review, case
examples and broad discussion among CHHS programs. Publishing data publicly is
always a balance between the protection of confidentiality and the usability of the data.
The project timeline for the CHHS DDG Workgroup is below:
3/15/15 Planning Meeting Part 1 – Participants included DHCS, CDPH,
OSHPD, OHII
3/20/15 Planning Meeting Part 2 – Participants included DHCS, CDPH,
OSHPD, OHII
4/7/15 Present Objectives for the project and use the DHCS PAR-DBR as an
example
4/23/15 Presentations from OSHPD and CDPH regarding current processes
and approach to small cell sizes
5/5/15 Discuss concept of uniqueness as a way to measure risk for re-
identification and gather input from Departments/Offices regarding
DDG variables and topics
5/27/15 Review initial draft DDG – Focus on new sections of the document
6/8/15 Review initial draft DDG – Focus on Data Assessment for Public
Release Procedure
May & Meet with each department/office individually
June, 2015

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 49 of 68
6/30/15 Review draft DDG version 0.2
July 2015 Departments/offices vet the DDG within their departments/offices
8/21/15 Received input from the CHHS Risk Management Committee
8/6/15 Review draft DDG version 0.3
9/14/15 Progress update for DDG Workgroup and discussion of additional
topics
12/18/15 Presentation from NORC to review their findings of the draft DDG
1/8/16 Receive final recommendations from NORC
Jan. 2016 Provide DDG version 0.4 to DDG Workgroup
2/18/16 Review and discussion of draft DDG version 0.4 with the DDG
Workgroup
3/18/16 Provide DDG version 0.5 with outstanding comments from the DDG
Workgroup to the Data Subcommittee
4/18/16 Provide revised draft DDG to the Data Subcommittee.
5/24/16 Provide draft DDG version 0.7 from the CHHS Data Subcommittee to
the CHHS Advisory Council. The Advisory Council shared the DDG
version 0.7 with the other subcommittees and discussed the version
0.7 at the 6/8/16 meeting and the version 0.8 at the 7/6/16 meeting.
7/7/16 Provide draft DDG version 0.10 to the Undersecretary.
9/23/16 DDG approved by CHHS Undersecretary as Version 1.0.
The final document will be incorporated into the Open Data Handbook and made
publicly available.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 50 of 68
11) Legal Framework
The overarching legal framework for the CHHS Data De-identification Guidelines is the
California Information Practices Act, California Civil Code 1798 et seq., which was
established in 1977 and applies to all state government entities. The IPA includes
requirements for the collection, maintenance, and dissemination of any information that
identifies or describes an individual. The IPA and other California statutes limit the
disclosure of personal information, consistent with the California Constitutional right to
privacy. However, state agencies are generally permitted (and sometimes required
under the California Public Records Act and other laws) to disclose data that have been
de-identified. Summarized or aggregated data may still be identifiable; the DDG
provides Guidelines for assessing whether data have been de-identified.
While most state agencies are covered by the IPA, some are also covered by or
impacted by HIPAA. Unlike the IPA, which applies to all personal information, HIPAA
only applies to certain health or healthcare-related information. HIPAA requirements
apply in combination with IPA requirements.
“Personal Information” is defined by the California Civil Code section 1798.3(a) as “any
information that is maintained by an agency that identifies or describes an individual,
including, but not limited to,
his or her name,
social security number,
physical description,
home address,
home telephone number,
education,
financial matters, and
medical or employment history.
It includes statements made by, or attributed to, the individual.”
Under Section 1798.24 of the IPA, “An agency shall not disclose any personal
information in a manner that would link the information disclosed to the individual to
whom it pertains,” unless it is disclosed as described in Section 1798.24.
Senate Bill 13 updated the IPA, effective January 1, 2006, to require Committee for the
Protection of Human Subjects (CPHS) review and approval before personal information
(linkable to any individual) that is held by any state agency or department can be
released for research purposes. CPHS does not delegate reviews for compliance with
the IPA to other institutional review boards. (http://www.oshpd.ca.gov/Boards/CPHS/)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 51 of 68
California Laws Governing the Collection and Release of Confidential, Personal,
or Sensitive Information (please note that this is not an exhaustive list)
General State Collected Information and Data
Civ. Code 1798.24, 1798.24a, 1798.24b (all personal information including
health data)
Gov. Code 11015.5 (electronically collected personal information)
General Medical Data
Civ. Code 56.10 – 56.11
Civ. Code 56.13
Civ. Code 56.29
Health & Saf. Code 128730
Health & Saf. Code 128735
Health & Saf. Code 128736
Health & Saf. Code 128737
Health & Saf. Code 128745
Health & Saf. Code 128766
Birth Defects
Health & Saf. Code 103850
Blood Lead Analysis
Health & Saf. Code 124130
Cancer
Health & Saf. Code 104315
Health & Saf. Code 103875
Health & Saf. Code 103885
Child Health Information
Health & Saf. Code 130140.1
Child Health Screening
Health & Saf. Code 124110
Health & Saf. Code 124991

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 52 of 68
Cholinesterase Testing
Health & Saf. Code 105206
Developmentally Disabled
Health & Saf. Code 416.18
Health & Saf. Code 416.8
Welf. & Inst. Code 4514, 4514.3, 4514.5
Welf. & Inst. Code 4517 (aggregation and publication of data)
Welf. & Inst. Code 4744
Welf. & Inst. Code 4659.22
Environmental Health Hazards
Health & Saf. Code 59016
General Public Health Records
Health & Saf. Code 121035
Health & Saf. Code 100330
Genetic Information
Health & Saf. Code 124975
Health & Saf. Code 124980
Health & Saf. Code 125105 (prenatal test)
Civ. Code 56.17
HIV/AIDS
Health & Saf. Code 121022
Health & Saf. Code 121023
Health & Saf. Code 121025
Health & Saf. Code 121075
Health & Saf. Code 121085
Health & Saf. Code 121110
Health & Saf. Code 121125
Health & Saf. Code 121010
Health & Saf. Code 120820
Health & Saf. Code 120980
Health & Saf. Code 121280
Health & Saf. Code 120962

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 53 of 68
Health & Saf. Code 120975
Health & Saf. Code 121080
Health & Saf. Code 121090
Health & Saf. Code 121095
Health & Saf. Code 121120
Rev. & T. Code 19548.2
Immunizations
Health & Saf. Code 120440
Independent Medical Review
Health & Saf. Code 1374.33
Involuntary Mental Health (LPS covered records)
Welf. & Inst. Code 5328 through 5328.9
Welf. & Inst. Code 5329 (aggregation and publication of data)
Welf. & Inst. Code 5540
Welf. & Inst. Code 5610
Welf. & Inst. Code 4135
Educ. C. 56863
Medi-Cal Data
Welf. & Inst. Code 14100.2
Welf. & Inst. Code 14015.8
Welf. & Inst. Code 14101.5
Parkinson’s Disease Registry
Health & Saf. Code 103865
Payment and Billing Info
Health & Saf. Code 440.40 (applies only to GACHs)
Prenatal Tests
Health & Saf. Code 120705
Health & Saf. Code 125105

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 54 of 68
Public Assistance
Welf. & Inst. Code 10850 (Confidential Information)
Public Social Services
Welf. & Inst. Code 10850
Substance Abuse Treatment Data
Health & Saf. Code 11845.5
Health & Saf. Code 11812
Vital Records
Health & Saf. Code 102430
Health & Saf. Code 102425
Health & Saf. Code 102426
Health & Saf. Code 102455
Health & Saf. Code 102460
Health & Saf. Code 102465
Health & Saf. Code 102475
Health & Saf. Code 103025
Federal Laws Governing Public Data Release
(please note that this is not an exhaustive list)
HIPAA - Section 164.514 of the HIPAA Privacy Rule (45 CFR)
42 CFR Part 2
Family Educational Rights and Privacy Act (FERPA) (20 U.S.C. § 1232g; 34 CFR
Part 99)
Freedom of Information Act (FOIA) (5 U.S.C. § 552)
Data De-identification
While the IPA does not include specific de-identification methods or criteria, the basic
concept of statistical de-identification has no different meaning, and the basic standard
of protection of identifiable data is no different for IPA covered PI than for HIPAA
covered PHI.
The California Office of Health Information Integrity (CalOHII) is authorized by state
statute to coordinate and monitor HIPAA compliance by all California State entities
within the executive branch of government covered or impacted by HIPAA. The 2014
assessment that was revised July 2015, identified programs and departments in CHHS

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 55 of 68
that are considered covered entities under HIPAA as a Health Care Provider, Health
Care Plan, Health Care Clearinghouse, Hybrid Entity or Business Associate. Detail is
provided in Appendix B. One difference between CA IPA and HIPAA is the
documentation requirement in HIPAA for data de-identified using the Expert
Determination method. Each of the following departments will need to identify which
programs within the department are impacted by HIPAA as part of the department
specific DDG.
Department of Aging
Department of Developmental Services
Department of Health Care Services
Department of Managed Health Care
Department of Public Health
Department of Social Services
Department of State Hospitals
Health and Human Services Agency
Office of Systems Integration
For programs and departments that are covered by HIPAA, de-identification must meet
the HIPAA standard. The DDG serves as a tool to make and document an expert
determination consistent with the HIPAA standard. The following comes from federal
guidance for HIPAA that provides more detail regarding Safe Harbor and Expert
Determination under the HIPAA standard.
The HIPAA Standard
31
for de-identification of protected health information (PHI)
32
states
“Health information that does not identify an individual and with respect to which there is
no reasonable basis to believe that the information can be used to identify an individual
is not individually identifiable health information.” If the data are de-identified, and it is
not reasonably likely that the data could be re-identified, the Privacy Rule no longer
restricts the use or disclosure of the de-identified data.
The following is quoted from the “Guidance Regarding Methods for De-identification of
Protected Health Information in Accordance with the Health Insurance Portability and
Accountability Act (HIPAA) Privacy Rule”, published November, 2012 by the U.S.
Department of Health & Human Services, Office for Civil Rights:
(http://www.hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/De-
31
The Standard is found in the HIPAA Privacy Rule, 45 CFR section 164.514(a).
32
“PHI” is defined as information which relates to the individual’s past, present, or future physical or
mental health or condition, the provision of health care to the individual, or the past, present, or future
payment for the provision of health care to the individual, and that identifies the individual, or for which
there is a reasonable basis to believe can be used to identify the individual. (45 CFR section 160.103)

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 56 of 68
identification/guidance.html) (Formatting of text may be different than the original
document.)
The HIPAA De-identification Standard
Section 164.514(a) of the HIPAA Privacy Rule (45 CFR) provides the standard for de-
identification of protected health information. Under this standard, health information
is not individually identifiable if it does not identify an individual and if the covered
entity has no reasonable basis to believe it can be used to identify an individual.
§ 164.514 Other requirements relating to uses and disclosures of protected health
information.
(a) Standard: de-identification of protected health information. Health information
that does not identify an individual and with respect to which there is no reasonable
basis to believe that the information can be used to identify an individual is not
individually identifiable health information.
Sections 164.514(b) and(c) of the Privacy Rule contain the implementation
specifications that a covered entity must follow to meet the de-identification
standard. As summarized in Figure 1, the Privacy Rule provides two methods by
which health information can be designated as de-identified.
Figure 1. Two methods to achieve de-identification in accordance with the HIPAA
Privacy Rule.
The first is the “Expert Determination” method:
(b) Implementation specifications: requirements for de-identification of protected
health information. A covered entity may determine that health information is not
individually identifiable health information only if:

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 57 of 68
(1) A person with appropriate knowledge of and experience with generally accepted
statistical and scientific principles and methods for rendering information not
individually identifiable:
(i) Applying such principles and methods, determines that the risk is very small that
the information could be used, alone or in combination with other reasonably
available information, by an anticipated recipient to identify an individual who is a
subject of the information; and
(ii) Documents the methods and results of the analysis that justify such
determination; or
The second is the “Safe Harbor” method:
(2)(i) The following identifiers of the individual or of relatives, employers, or
household members of the individual, are removed:
(A) Names
(B) All geographic subdivisions smaller than a state, including street address, city,
county, precinct, ZIP code, and their equivalent geocodes, except for the initial three
digits of the ZIP code if, according to the current publicly available data from the
Bureau of the Census:
(1) The geographic unit formed by combining all ZIP codes with the same three
initial digits contains more than 20,000 people; and
(2) The initial three digits of a ZIP code for all such geographic units containing
20,000 or fewer people is changed to 000
(C) All elements of dates (except year) for dates that are directly related to an
individual, including birth date, admission date, discharge date, death date, and all
ages over 89 and all elements of dates (including year) indicative of such age,
except that such ages and elements may be aggregated into a single category of
age 90 or older
(D) Telephone numbers
(E) Fax numbers
(F) Email addresses
(G) Social security numbers
(H) Medical record numbers

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 58 of 68
(I) Health plan beneficiary numbers
(J) Account numbers
(K) Certificate/license numbers
(L) Vehicle identifiers and serial numbers, including license plate numbers
(M) Device identifiers and serial numbers
(N) Web Universal Resource Locators (URLs)
(O) Internet Protocol (IP) addresses
(P) Biometric identifiers, including finger and voice prints
(Q) Full-face photographs and any comparable images
(R) Any other unique identifying number, characteristic, or code, except as permitted
by paragraph (c) of this section [Paragraph (c) is presented below in the section “Re-
identification”]; and
(ii) The covered entity does not have actual knowledge that the information could be
used alone or in combination with other information to identify an individual who is a
subject of the information.
Satisfying either method would demonstrate that a covered entity has met the
standard in §164.514(a) above. De-identified health information created following
these methods is no longer protected by the Privacy Rule because it does not fall
within the definition of PHI. Of course, de-identification leads to information loss
which may limit the usefulness of the resulting health information in certain
circumstances. As described in the forthcoming sections, covered entities may wish
to select de-identification strategies that minimize such loss.
Re-identification
The implementation specifications further provide direction with respect to re-
identification, specifically the assignment of a unique code to the set of de-identified
health information to permit re-identification by the covered entity.
(c) Implementation specifications: re-identification. A covered entity may assign a
code or other means of record identification to allow information de-identified under
this section to be re-identified by the covered entity, provided that:

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 59 of 68
(1) Derivation. The code or other means of record identification is not derived from or
related to information about the individual and is not otherwise capable of being
translated so as to identify the individual; and
(2) Security. The covered entity does not use or disclose the code or other means of
record identification for any other purpose, and does not disclose the mechanism for
re-identification.
If a covered entity or business associate successfully undertook an effort to identify
the subject of de-identified information it maintained, the health information now
related to a specific individual would again be protected by the Privacy Rule, as it
would meet the definition of PHI. Disclosure of a code or other means of record
identification designed to enable coded or otherwise de-identified information to be
re-identified is also considered a disclosure of PHI.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 60 of 68
12) Abbreviations and Acronyms
CalOHII ....... California Office of Health Information Integrity
CDC ............ Centers for Disease Control and Prevention
CDPH .......... California Department of Public Health
CDSS .......... Department of Social Services
CHHS .......... California Health and Human Services Agency
CMS ............ Centers for Medicare and Medicaid Services
CPHS .......... Committee for the Protection of Human Subjects
DDG ............ Data De-Identification Guidelines
DHCS ......... Department of Health Care Services
HIPAA ......... Health Insurance Portability and Accountability Act
IPA .............. Information Practices Act
MHSOAC .... Mental Health Services Oversight and Accountability Commission
OSHPD ....... Office of Statewide Health Planning and Development
PAR-DBR .... Public Aggregate Reporting - DHCS Business Reports
PHI .............. Protected Health Information
PI ................. Personal Information
PRA ............. Public Records Act
PRT ............. Peer Review Team

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 61 of 68
13) Definitions
Aggregate – formed or calculated by the combination of many separate units or items
(Oxford Dictionary).
De-identified – generally defined under the HIPAA Privacy Rule (45 CFR section
164.514) as information (1) that does not identify the individual and (2) for which there is
no reasonable basis to believe the individual can be identified from it.
Denominator – the portion of the overall population being referenced in a table or a
figure representing the total population in terms of which statistical values are
expressed (Oxford Dictionary).
Numerator – the number of specific cases as identified by the variable from a given
population or the number above the line in a common fraction showing how many of the
parts indicated by the denominator are taken (Oxford Dictionary).
Protected Health Information – information which relates to the individual’s past,
present, or future physical or mental health or condition, the provision of health care to
the individual, or the past, present, or future payment for the provision of health care to
the individual, and that identifies the individual, or for which there is a reasonable basis
to believe can be used to identify the individual (HIPAA, 45 CFR section 160.103).
Personal Information – includes information that is maintained by an agency which
identifies or describes an individual, including his or her name, social security number,
physical description, home address, home telephone number, education, financial
matters, email address and medical or employment history. It includes statements
made by, or attributed to, the individual (California Civil Code section 1798.3).
Publishable State Data – Data is Publishable State Data if it meets one of the following
criteria: (1) data that are public by law such as via the PRA or (2) the data are not
prohibited from being released by any laws, regulations, policies, rules, rights, court
order, or any other restriction. Data shall not be released if it is highly restricted due to
the Health Insurance Portability and Accountability Act (HIPAA), state or federal law
(such data are defined as Level 3 later in this handbook).
33
Re-Identified – matching de-identified, or anonymized, personal information back to the
individual.
33
http://chhsopendata.github.io/

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 62 of 68
14) References
Armstrong, MP, G Rusthon, and DL Zimmerman, 1999, Geographically Masking Health
Data to Preserve Confidentiality. Statistics in Medicine, 18, 497-525.
Bambauer, Jane R., Tragedy of the Data Commons (March 18, 2011). Harvard Journal
of Law and Technology, Vol. 25, 2011. Available at SSRN:
http://ssrn.com/abstract=1789749 or http://dx.doi.org/10.2139/ssrn.1789749
Benitez K1, Malin B., Evaluating re-identification risks with respect to the HIPAA privacy
rule. J Am Med Inform Assoc. 2010 Mar-Apr;17(2):169-77. doi:
10.1136/jamia.2009.000026. http://www.ncbi.nlm.nih.gov/pubmed/20190059
CHHS Open Data Handbook - http://chhsopendata.github.io/
CHHS, Information Strategic Plan 2016.
Colorado Department of Public Health and Environment. “Guidelines for Working with
Small Numbers.” Retrieved from
http://www.cohid.dphe.state.co.us/smnumguidelines.html
Committee for the Protection of Human Subjects (CPHS), CPHS Bulletin & Update,
January, 2005.
Federal Committee on Statistical Methodology, Interagency Confidentiality and Data
Access Group. “Checklist on Disclosure Potential of Proposed Data Releases.”
Washington: Statistical Policy Office, Office of Management and Budget, July
1999.
Federal Committee on Statistical Methodology, “Statistical Policy Working Paper 22 –
Report on Statistical Disclosure Limitation Methodology.” Washington: Statistical
Policy Office, Office of Management and Budget, 1994.
Golle, Philippe. “Revisiting the uniqueness of simple demographics in the US
population. In Proceedings of the 5th ACM Workshop on Privacy in the Electronic
Society. ACM Press, New York, NY. 2006: 77-80.
Howe, H. L., A. J. Lake, and T. Shen. "Method to Assess Identifiability in Electronic
Data Files." American Journal of Epidemiology 165.5 (2006): 597-601. Print.
NAHDO-CDC Cooperative Agreement Project CDC Assessment Initiative. “Statistical
Approaches for Small Numbers: Addressing Reliability and Disclosure Risk.”
December 2004. Retrieved from
http://api.ning.com/files/sCi4ZnrAubmkUqLO5Zfm3XYlq*7jctjEJXwGDDMepE4_/
Statapproachesforsmallnumbers.pdf

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 63 of 68
NCHS Staff Manual on Confidentiality. Hyattsville, MD: National Center for Health
Statistics, Department of Health and Human Services, “NCHS Staff Manual on
Confidentiality.” 2004. Retrieved from
http://www.cdc.gov/nchs/data/misc/staffmanual2004.pdf.
NORC, “Case Study: The Disclosure Risk Implications of Small Cells Combined with
Multiple Tables or External Data,” January 8, 2016.
NORC, “NORC Recommendations for California Department of Health Care Services
(DHCS) Data De-Identification Guidelines (DDG),” January 8, 2016.
North American Association of Central Cancer Registries (NAACCR), “Using
Geographic Information Systems Technology in the Collection, Analysis, and
Presentation of Cancer Registry Data: A Handbook of Basic Practices,” October
2002.
Office of Civil Rights, U.S. Department of Health & Human Services. "Guidance
Regarding Methods for De-identification of Protected Health Information in
Accordance with the Health Insurance Portability and Accountability Act (HIPAA)
Privacy Rule." November 26, 2012. Retrieved from
http://www.hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/De-
identification/hhs_deid_guidance.pdf.
Ohio Department of Public Health. “Data Methodology for Public Health Practice.”
http://www.odh.ohio.gov/~/media/ODH/ASSETS/Files/data%20statistics/standard
s/methodological%20standards/disclimit.ashx.
Panel on Disclosure Review Boards of Federal Agencies: Characteristics, Defining
Qualities and Generalizability, 2000, Proceedings of the Joint Statistical
Meetings, Indianapolis, Indiana.
Privacy Technical Assistance Center, U.S. Department of Education. “Data De-
identification: An Overview of Basic Terms.” May 2013. Retrieved from
http://ptac.ed.gov/sites/default/files/data_deidentification_terms.pdf
State of California, Department of Finance, Report P-1 (Race): State and County
Population Projections by Race/Ethnicity, 2010-2060. Sacramento, California,
January 2013. Retrieved from http://www.dhcs.ca.gov/services/MH/InfoNotices-
Ltrs/Documents/InfoNotice-PrimaryLang-Enclosure1.pdf
State of California, Department of Health Care Services, Trend in Medi-Cal Program
Enrollment by Managed Care Status - for Fiscal Year 2004-2012, 2004-07 -
2012-07, Report Date: July 2013. Retrieved from

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 64 of 68
http://www.dhcs.ca.gov/dataandstats/statistics/Documents/1_6_Annual_Historic_
Trend.pdf
Stoto, MA. Statistical Issues in Interactive Web-based Public Health Data Dissemination
Systems. RAND Health. September 19, 2002.
Sweeney, L. “Information Explosion, Confidentiality, Disclosure, and Data Access:
Theory and Practical Applications for Statistical Agencies,” L Zayatz, P Doyle, J
Theeuwes and J Lane (eds), Urban Institute, Washington, DC, 2001.
Sweeney, L. “K-anonymity: a model for protecting privacy.” International Journal of
Uncertainty, Fuzziness, and Knowledge-Based Systems. 2002; 10(5): 557-570.
Sweeney, L. Testimony before that National Center for Vital and Health Statistics
Workgroup for Secondary Uses of Health information. August 23, 2007.
The Centers for Medicare and Medicaid Services, Office of Information Products and
Data Analytics. “Medicare Fee-For Service Provider Utilization & Payment Data
Physician and Other Supplier Public Use File: A Methodological Overview.” April
7, 2014.
Washington State Department of Health. "Guidelines for Working with Small Numbers."
N.p., 15 October 2012. Retrieved from
http://www.doh.wa.gov/Portals/1/Documents/5500/SmallNumbers.pdf.

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 65 of 68
15) Appendix A: Expert Determination Template
HIPAA covered entities in CHHS must de-identify data in compliance with the HIPAA
standard. Under the HIPAA standard, either Safe Harbor or Expert Determination must
be used. If Expert Determination is used then the documentation of the review is
essential. The following may serve as a template for this documentation with the
reference to the CHHS DDG to support the analysis documented.
Documentation of Expert Determination Template
Name of Report:
Reason for Data Release:
Identify why the data release does not meet Safe Harbor. For example:
The request does not meet the Safe Harbor standard because it includes counts by
county (geographic area smaller than the state) or counts by month (which does not
meet the criteria for dates). Therefore, the steps in the CHHS DDG are being used to
assess the tables.
Document how the conditions of each step are met or not
met
Result
Step 1 – Presence of Personal Characteristics
Summary:
Step 2 – Numerator Denominator Condition
Summary:
Step 3 – Assess Potential Risk
Summary:
Step 4 – Statistical Masking
Summary:
Step 5 – Expert Review
Summary:
“Risk is very small that the information could be used, alone or in
combination with other reasonably available information, by an anticipated
recipient to identify an individual who is a subject of the information”

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 66 of 68
16) Appendix B: 2015 HIPAA Reassessment Results
The CalOHII is authorized by state statute to coordinate and monitor HIPAA
compliance by all California State entities within the executive branch of government
covered or impacted by HIPAA. To help ensure full compliance with HIPAA, CalOHII
conducted a reassessment with all State Departments in January 2014 and updated as
of July 27, 2015.
34
The following are the self-reported results of this reassessment:
DEPARTMENTS
COVERED ENTITIES
IMPACTED
ENTITIES
Health Care
Provider
Health Care Plan
Health Care
Clearinghouse
Hybrid Entity
Business
Associate
Trading Partner
Impacted by Data
Content
Health Oversight
Agency
COVERED ENTITIES & BUSINESS ASSOCIATES
1
Aging, Department of
X
X
2
Controllers Office, State
X
3
Corrections and Rehabilitation, CA Dept. of,
X
X
4
Developmental Services, Dept. of
X
X
X
X
X
X
X
5
Forestry and Fire Protection, Dept. of
X
6
Health and Human Services Agency
X
X
X
7
Healthcare Services, Department of
X
X
X
X
8
Justice, Department of
X
9
Managed Health Care, Dept. of
X
X
10
Public Employees' Retirement System
X
X
X
X
11
Public Health, Department of
X
X
X
X
X
12
Social Services, Dept. of
X
13
State Hospitals, Dept. of
X
X
X
X
X
14
Systems Integration, Office of
X
15
Veterans Affairs, Dept. of (CalVET)
X
X
IMPACTED ENTITIES
1
Health Information Integrity, California Office of
X
2
Health Planning and Development, Office of Statewide
X
3
Industrial Relations, Dept. of
X
X
4
Insurance, Dept. of
X
5
Inspector General, Office of
X
34
http://www.ohi.ca.gov/calohi/download2011-HIPAA%20Assessment%20Results%207-27-2015.pdf

CHHS Data De-Identification Guidelines (DDG) Page 67 of 68
17) Appendix C: State and County Population Projections
The following table is provided for reference related to the race and ethnicity
composition at the county level. It is State of California, Department of Finance, Report
P-1 (Race): State and County Population Projections by Race/Ethnicity, 2010-2060.
Sacramento, California, January 2013. The table is for year 2010.
State/
County
Race/Ethnicity
Total (All
race
groups)
White, not
Hispanic
or Latino
Black,
not
Hispanic
or Latino
Americ
an
Indian,
not
Hispani
c or
Latino
Asian,
not
Hispanic
or Latino
Native
Hawaiia
n and
other
Pacific
Islander,
not
Hispanic
or
Latino
Hispanic
or Latino
Multi-
Race,
not
Hispani
c or
Latino
California
37,309,382
15,024,945
2,188,296
163,040
4,827,438
131,415
14,057,596
916,651
Alameda
1,513,236
514,086
186,737
4,098
395,898
12,337
343,141
56,939
Alpine
1,163
869
0
204
2
0
71
17
Amador
37,853
30,091
950
539
447
53
4,859
913
Butte
219,990
164,870
3,139
3,376
9,458
397
31,670
7,080
Calaveras
45,462
37,999
353
518
526
59
4,779
1,227
Colusa
21,478
8,601
153
284
247
50
11,892
251
Contra
Costa
1,052,211
508,220
93,096
3,033
149,853
4,532
256,047
37,431
Del Norte
28,544
18,522
1,060
1,928
933
21
5,126
953
El Dorado
180,921
143,909
1,289
1,543
6,739
248
22,443
4,750
Fresno
932,377
307,295
45,680
6,080
86,637
1,067
469,935
15,682
Glenn
28,143
15,688
181
463
663
17
10,664
467
Humboldt
134,663
103,996
1,404
6,940
3,127
320
13,560
5,316
Imperial
175,389
24,406
5,359
1,639
1,954
75
140,945
1,010
Inyo
18,528
12,309
102
1,895
184
12
3,629
396
Kern
841,146
325,711
45,798
5,933
33,266
996
414,414
15,028
Kings
152,656
54,303
10,686
1,305
5,343
216
77,595
3,208
Lake
64,599
47,973
1,186
1,531
647
81
11,165
2,016
Lassen
35,136
23,452
2,999
992
427
153
6,243
870
Los
Angeles
9,824,906
2,746,305
821,829
19,527
1,336,086
23,152
4,694,972
183,035
Madera
151,328
57,494
5,204
1,818
2,661
98
81,807
2,246
Marin
252,731
184,377
7,069
520
14,004
423
39,459
6,879
Mariposa
18,193
15,224
118
456
158
21
1,677
539
Mendocin
o
87,924
60,398
544
3,433
1,469
79
19,691
2,310
Merced
255,937
83,475
8,742
1,134
17,363
466
140,472
4,286
Modoc
9,648
7,677
69
280
53
17
1,344
208
Mono
14,240
9,731
36
217
206
9
3,815
226
Monterey
416,259
136,348
11,334
1,372
24,430
1,882
231,700
9,193
Napa
136,811
77,088
2,457
533
9,377
299
44,235
2,823
Nevada
98,639
85,120
331
787
1,295
83
8,703
2,320
Orange
3,017,327
1,336,843
45,894
6,247
540,485
8,507
1,010,752
68,599

CHHS Data De-Identification Guidelines (DDG) Version 1.0 Page 68 of 68
State/
County
Race/Ethnicity
Total (All
race
groups)
White, not
Hispanic
or Latino
Black,
not
Hispanic
or Latino
Americ
an
Indian,
not
Hispani
c or
Latino
Asian,
not
Hispanic
or Latino
Native
Hawaiia
n and
other
Pacific
Islander,
not
Hispanic
or
Latino
Hispanic
or Latino
Multi-
Race,
not
Hispani
c or
Latino
Placer
350,275
263,747
4,448
2,063
22,443
685
46,677
10,214
Plumas
19,911
16,989
173
453
98
14
1,602
581
Riverside
2,191,886
874,405
133,791
10,951
127,558
5,891
993,930
45,361
Sacramen
to
1,420,434
691,338
140,694
7,973
200,201
13,795
307,513
58,920
San
Benito
55,350
20,573
380
215
1,542
54
31,721
865
San
Bernardin
o
2,038,523
684,856
172,602
8,660
122,187
5,970
1,003,256
40,991
San Diego
3,102,745
1,501,675
148,728
14,121
333,728
13,606
999,392
91,494
San
Francisco
806,254
338,874
46,758
1,808
268,020
3,145
122,869
24,780
San
Joaquin
686,588
248,202
49,199
3,220
94,812
3,315
267,086
20,752
San Luis
Obispo
269,713
191,725
5,392
1,367
8,622
334
56,309
5,965
San
Mateo
719,729
303,475
19,474
1,134
178,665
10,225
184,420
22,337
Santa
Barbara
424,050
201,823
7,507
1,817
20,281
675
183,511
8,436
Santa
Clara
1,786,429
627,438
43,926
4,085
573,622
6,413
481,108
49,838
Santa
Cruz
263,260
156,796
2,357
972
11,260
288
84,804
6,783
Shasta
177,472
145,533
1,429
4,150
4,893
216
15,410
5,841
Sierra
3,230
2,883
4
34
3
2
258
48
Siskiyou
44,893
35,691
537
1,547
548
58
4,663
1,848
Solano
413,117
170,275
58,396
1,853
59,126
3,304
99,759
20,405
Sonoma
484,084
321,695
7,009
3,560
17,581
1,404
120,414
12,422
Stanislaus
515,205
243,208
12,534
2,894
24,168
3,170
216,228
13,003
Sutter
94,669
48,033
1,734
925
13,582
251
27,326
2,818
Tehama
63,487
45,708
347
1,213
548
53
14,010
1,610
Trinity
13,713
11,307
38
536
183
12
1,080
557
Tulare
443,066
145,549
5,505
3,319
13,543
370
269,012
5,767
Tuolumne
55,144
45,279
1,161
831
546
51
5,950
1,327
Ventura
825,077
402,144
13,216
2,363
55,015
1,351
333,230
17,758
Yolo
201,311
100,679
5,025
1,094
26,065
842
61,057
6,549
Yuba
72,329
42,666
2,134
1,260
4,659
256
18,192
3,162
