
Milwaukee County Department of Human Resources — Employee Benefits
Milwaukee County Courthouse • 901 N. 9th St. • Milwaukee, WI 53233 • (414) 278-4198
MEDICAL PLAN
DENTAL PLAN
VISION PLAN
LIFE INSURANCE
LEGAL PLAN
FLEXIBLE SPENDING
ACCOUNT
RETIREMENT
BENEFITS
SHORT-TERM
DISABILITY
DEFERRED
COMPENSATION
WELLNESS
PROGRAM
MILWAUKEE COUNTY
BENEFITS
2020
MEDICAL PLAN
DENTAL PLAN
VISION PLAN
LIFE INSURANCE
LEGAL PLAN
FLEXIBLE SPENDING
ACCOUNT
RETIREMENT
BENEFITS
SHORT-TERM
DISABILITY
DEFERRED
COMPENSATION
WELLNESS
PROGRAM

Milwaukee County 2020 Benefits | 3
TOTAL REWARDS
Introduction & 2020 Benefit Plan Overview.......................................................................................... 5
Summary of Status Changes................................................................................................................. 8
2020 Medical Insurance........................................................................................................................ 9
2020 Medical Plan Coverage At-A-Glance .................................................................................. 10
Employee Bi-Weekly Medical Premium Contributions ................................................................ 12
2020 Dental Insurance ........................................................................................................................ 17
2020 Dental Plan Coverage At-A-Glance ..................................................................................... 17
Employee Bi-Weekly Dental Premium Contributions ................................................................... 18
2020 Vision Benefit ............................................................................................................................. 20
2020 Vision Benefit Coverage At-A-Glance ................................................................................. 20
Employee Bi-Weekly Vision Premium Contributions ................................................................... 21
Flexible Spending Accounts ................................................................................................................ 22
Life Insurance Plans ............................................................................................................................ 29
Legal Plan ............................................................................................................................................ 33
Milwaukee County Benefit Enrollment System .................................................................................. 34
How To Enroll Online: A Screen-by-Screen Guide ................................................................... 35
Short-Term Disability .......................................................................................................................... 38
Commuter Value Pass ......................................................................................................................... 40
Employee Assistance Program............................................................................................................ 41
Employee Discount Program ............................................................................................................... 42
Tuition Reimbursement Program ......................................................................................................... 43
Wellness Program ............................................................................................................................... 44
Mandatory Direct Deposit of Payroll Checks ...................................................................................... 48
Retirement Benefits ............................................................................................................................ 49
Deferred Compensation Plan .............................................................................................................. 51
Annual Notices.................................................................................................................................... 52
Table of Contents

4 | Milwaukee County 2020 Benefits
TOTAL REWARDS

Milwaukee County 2020 Benefits | 5
TOTAL REWARDS
Welcome to Milwaukee County! Milwaukee County recognizes that employees have different needs. That’s why
we offer a benefit program that allows you to choose among a number of benefit options. You can select from these
options to design the benefit plan that’s right for you.
You are encouraged to carefully consider your personal situation as you evaluate your benefit choices. Milwaukee
County benefits include:
• Health Insurance.
• Dental Insurance.
• Vision Insurance.
• Group Life Insurance.
• Legal Plan.
• Flexible Spending Accounts (FSA).
• Employee Assistance Program (EAP).
• Deferred Compensation (457 Plan).
• Short-Term Disability Plan.
• Commuter Value Pass Program.
The information in this booklet provides a summary of your benefits under the County-offered benefit plans. For more
detailed information along with notices of your legal rights, review each plan’s Summary Plan Description (SPD)
booklet. The booklets are available through the Milwaukee County website.
In the case of conflict between the information presented in this benefit booklet and the plan’s SPD booklets, the plan’s
SPD booklets determine the coverage.
Employee Eligibility
All Milwaukee County employees appointed to a position with an authorized work week of 20 hours or more and not
excluded by job code or ordinance are eligible to enroll in any benefit plan that is offered by Milwaukee County.
Dependent Eligibility
An eligible dependent is considered to be:
• Your legally married spouse (same or opposite-
sex), you or your spouse’s child who is under age
27, including a natural child, stepchild, a legally
adopted child, a child placed for adoption or a child
for whom you or your spouse are the legal guardian.
• An unmarried child of any age who is or becomes
disabled and dependent upon you.
• A child of a dependent child (until the dependent
who is the parent turns 18).
To be eligible for coverage under the plan, a dependent
must reside within the United States.
2020 Benefit Plan Overview
PROOF OF ALL DEPENDENTS’
ELIGIBILITY IS REQUIRED
If you elect to cover a dependent under Milwaukee
County’s health, dental or vision insurance, you will
be contacted by a third party dependent verification
service to provide documentation that you are
covering an eligible dependent. Please mark/
black out any personal financial information on the
copies of your documents before you submit them
for verification.

6 | Milwaukee County 2020 Benefits
TOTAL REWARDS
The definition of dependent is subject to the following conditions and limitations:
• A dependent includes any dependent child under 27 years of age who is not eligible for coverage under a group
health benefit plan offered by their employer and for whom the amount of the dependent’s premium contribution is
no greater than the premium amount for his or her coverage as a dependent under the participant’s plan.
A child who meets the requirements set forth above ceases to be eligible as a dependent on the last day of the month
of the child’s 27th birthday.
A dependent also includes a child for whom health care coverage is required through a Qualified Medical Child Support
Order or other court or administrative order.
Effective Date of Insurances
The following insurances become effective the first of the month following your hire date:
• Health Insurance.
• Dental Insurance.
• Vision Insurance.
• Legal Plan.
• Flexible Spending Accounts (FSA).
• Short-Term Disability.
• Employee Assistance Plan (EAP).
• Commuter Value Pass Program.
If elected, basic life insurance and optional term insurance will begin on the first of the month following six months of
continuous employment.
For example, If you were hired on April 11, your insurance coverage begins on May 1 and the basic life insurance and
optional term insurance coverage begins on November 1.
Employees must enroll within 30 days from their hire date. If an employee does not enroll during their 30-day window,
he or she must wait until the following open enrollment period to enroll in benefits for the following year.
Premiums for your insurance coverage are deducted over 26 pay periods.
$500 Opt-Out Award
Eligible employees can choose to waive medical coverage through Milwaukee County if they have group coverage
through a spouse or other employment. Waiver elections can be completed online in the Benefit Enrollment System.
IMPORTANT INFORMATION
• You must enter the name of your other insurance in the Benefit Enrollment System in order to be eligible for the
$500 opt-out award.
• The lump-sum taxable $500 opt-out award will be paid on a paycheck with a separate direct deposit issued just
prior to April 1 of each year. Opt-outs after April 1 will be paid out quarterly.
• To be eligible for the award, the employee must waive medical coverage for the entire plan year.
• Re-entry for medical coverage between annual open enrollment periods is allowed with proof of involuntary loss

Milwaukee County 2020 Benefits | 7
TOTAL REWARDS
of coverage through the other group plan due to termination of employment, layoff, legal separation or divorce,
death of spouse or retirement.
• The full $500 award must be returned in the event you terminate employment, retire or enroll in a
Milwaukee County health plan.
Special Enrollment Notice
If you are declining enrollment for yourself or your dependents (including your spouse) because of other health
insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or
your dependents lose eligibility for that other coverage. However, you must request enrollment within 30 days after
your or your dependents’ other coverage ends.
In addition, if you have a new dependent as a result of marriage, birth, adoption or placement for adoption, you may be
able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage,
birth, adoption or placement for adoption.
Annual Open Enrollment
Each year in the fall, a two-week period is designated as the Open Enrollment period. Elections made during Open
Enrollment are effective January 1 of the following year.
The following is a partial list of what you can do during the Open Enrollment period each year:
• Add or remove coverage.
• Add or remove dependents.
• Increase, decrease or request optional life insurance coverage.
• Participate in the Flexible Spending Account.
COBRA
COBRA, the Consolidated Omnibus Budget Reconciliation Act, is a federal law that permits eligible employees and
dependents whose medical, dental and/or vision insurance would otherwise terminate to continue coverage for specific
periods of time under certain conditions.
• Employees may continue single or family coverage through Milwaukee County for a maximum of 18 months if:
• Employment is terminated (including lay-offs) for any reason other than the employee’s gross misconduct.
• Or, the employee’s work hours are reduced or work status is changed such that the employee is no longer
eligible for coverage.
• Dependents may continue their coverage through Milwaukee County for a maximum of 36 months if coverage is
terminated:
• Due to the death of the employee.
• Or, due to divorce or legal separation of the dependent from the employee.
• Or, with respect to a dependent child, the child is no longer eligible as a dependent under Milwaukee
County’s eligibility rules.

8 | Milwaukee County 2020 Benefits
TOTAL REWARDS
If you experience the
following life/family event:
You may make the following change(s)
within 30 days of the event:
YOU MAY NOT
make these
types of changes:
Marriage
• Enroll yourself, if applicable.
• Enroll your new spouse and other eligible dependents.
• Drop health coverage (to enroll in your spouse’s plan).
• Change health plans.
• Drop health coverage and
not enroll in spouse’s plan.
Divorce
• Drop your spouse from your health coverage.
• Enroll yourself and your dependent children if you
were previously enrolled in your spouse’s plan.
• Drop health coverage for
yourself.
Gain a child due to birth
or adoption (effective date
of birth or adoption placement)
• Enroll yourself, if applicable.
• Enroll the eligible child and any other eligible
dependents.
• Drop health coverage
for yourself or any other
covered individuals.
Child requires coverage
due to a QMCSO
• Add child named on QMCSO to your health coverage
(enroll yourself, if applicable and not already enrolled).
• Make any other changes,
except as required by the
QMCSO.
Loss of a child’s eligibility
(e.g., child reaches the
maximum age for coverage)
• Drop the child who lost eligibility from your health
coverage. Child will be offered COBRA.
• Drop health coverage
for yourself or any other
covered individuals.
Covered person has become
entitled to (or lost entitlement
to) Medicare or Medicaid
• Drop coverage for the person who became entitled to
Medicare or Medicaid.
• Add the person who lost entitlement to Medicare or
Medicaid.
• Drop health coverage
for yourself or any other
covered individuals who
are not newly Medicare or
Medicaid eligible.
Spouse obtains health
benefits in another group
health plan
• Drop your spouse from your health coverage.
• Drop your dependent children from your health
coverage.
• Drop coverage for yourself.
• Add any eligible dependents
to your health coverage.
Spouse loses employment,
experiences a termination
of their employer’s
contribution, or otherwise
loses coverage for health
benefits in another group
health plan
• Enroll your spouse and eligible dependent children in
your health plan.
• Enroll yourself if previously not enrolled because you
were covered under your spouse’s plan.
• Drop health coverage
for yourself or any other
covered dependents.
You return from military leave
• Enroll yourself.
• Enroll your spouse and other eligible dependents.
You become newly eligible for
benefits due to change
in employment status
• Enroll yourself.
• Enroll your spouse and other eligible dependents.
Summary of Common Change of Status Events
and Mid-Year Enrollment
CHANGES ALLOWED FOR EMPLOYEES UNDER BENEFIT PLANS
This chart is only a summary of some of the permitted changes and is not all inclusive.

Milwaukee County 2020 Benefits | 9
TOTAL REWARDS
Choice Plus Plan (PPO Comparable)
As a Preferred Provider Organization (PPO) participant:
• You can choose which doctor or specialist to see and an in-network or out-of-network provider. Note: you pay
substantially less when you go to a doctor in the network.
• You don’t need to select a primary care physician and you don’t need a referral to see a specialist.
Whether you choose an in-network or out-of-network provider, certain services require that you satisfy a copay,
deductible, and/or coinsurance. If you receive care from an out-of-network provider, your coverage will be at a lower
benefit level and you will have to pay a higher deductible and coinsurance.
2020 Medical Insurance
ADMINISTERED BY UNITEDHEALTHCARE
FINDING A UNITEDHEALTHCARE NETWORK PROVIDER
To confirm if your physician, hospital or other provider is included in the UnitedHealthcare network, or to find a
network physician, please contact UnitedHealthcare at the customer service number provided on the back cover
of this booklet, or confirm online using the following steps:
1. Go to www.myuhc.com and select the “Find Medical and Mental Health Providers and Facilities” link
located under the “Links and Tools” heading in the upper right corner.
2. Select the type of provider you are looking for (e.g., Medical Directory or Mental Health Directory).
3. Select the search criteria you want to search (e.g., Doctors, Clinics or Facilities).
4. Under the “Select a Plan” field, choose the “UnitedHealthcare Choice Plus” option for the PPO comparable
plan.
5. You can narrow the search by entering the provider’s name, but this step is optional.
6. Indicate the location where you would like to find providers (e.g., your zip code), and search by Health Care
by Category.
7. You may also narrow your search by gender and/or languages spoken by the provider or staff.
8. When you are finished entering your search criteria, indicate if you are searching for a specific specialty
on the next screen.
9. Click to view the results.

10 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Network Non-Network
Annual Deductible
Single:
EE+Child(ren):
EE+Spouse:
EE+Family:
$1,250
$1,500
$2,250
$2,500
Single:
EE+Child(ren):
EE+Spouse:
EE+Family:
$2,250
$2,750
$4,250
$4,750
Office Visits
$30 copay $60 copay
Office Visits-Specialist
$40 copay $80 copay
Inpatient Hospital
80% of eligible charges 60% of eligible charges
Outpatient Surgery
80% of eligible charges 60% of eligible charges
Emergency Room
$200 copay $200 copay
Preventive Services
100% of eligible charges 60% of eligible charges
Medical Out-of-Pocket
Maximum
Individual:
Aggregate Family:
$3,000
$6,000
Individual:
Aggregate Family:
$4,600
$9,200
Pharmacy Copay—Retail
(up to 30-day supply)
Tier One:
Tier Two:
Tier Three:
$10
$30
$50
Tier One:
Tier Two:
Tier Three:
$10
$30
$50
Pharmacy Copay—Mail
Order (up to 90-day supply,
required for mainetenance
medications)
Tier One:
Tier Two:
Tier Three:
$25
$75
$125
Tier One:
Tier Two:
Tier Three:
N/A
N/A
N/A
Specialty Pharmacy—Mail
Order (up to 30-day supply)
Tier Four: $75 Not covered
Pharmacy Out-of-Pocket
Maximum
Individual:
Aggregate Family:
$2,000
$4,000
Individual:
Aggregate Family:
$2,000
$4,000
2020 Medical Plan Coverage At-A-Glance
Note: this at-a-glance guide is intended as a summary only.
For specific terms, provisions, conditions, limitations or exclusions, please refer to the Summary Plan Description.

Milwaukee County 2020 Benefits | 11
TOTAL REWARDS
BENEFIT PLAN DEFINITIONS
Understanding how our plans work is a critical first step in taking action to manage costs. Keep these key benefit terms
in mind when comparing the plans and coverage available to you.
Coinsurance: This is the percentage of the cost you pay when you receive certain health care services. Example:
For in-network services under the County’s Choice Plus plan, plan participants pay 20% and the County pays 80% of
covered expenses for most services. The 20% share is the employee’s coinsurance.
Co-payment: This is the flat-dollar amount you pay when you receive certain medical care services. Co-pays are
typically due at the time you receive the service. Example: \enrollees in the plan pay a $30 primary care or $40 specialty
care co-pay for in-network doctor’s office visits.
Deductible: This is the amount you are required to pay each year before the plan begins to pay benefits. You begin
accumulating expenses toward the satisfaction of your deductible at the beginning of each benefit year (January 1).
Example: With each new benefit year, employees who elect self only coverage under the Choice Plus Plan pay the first
$1,250 toward services subject to the plan’s deductible. Employees who elect coverage for themselves, their spouse
and dependent children pay the first $1,250 per individual, up to a maximum of $2,500 per family, toward services
subject to the plan’s deductible.
In-Network: This is care or services provided by doctors, hospitals, labs or other facilities that participate in the
network of providers assembled by UnitedHealthcare. Generally, you pay less when you receive care in-network
because the providers in the network agree to charge a pre-negotiated, lower fee. This reduces your out-of-pocket
costs and the overall claims costs.
Out-of-Network: This is care or services furnished by doctors, hospitals, labs or other facilities that DO NOT
participate in the UnitedHealthcare’s provider network. If you are enrolled in the Choice Plus Plan and use an out-
of-network provider, your share of the cost is based on the reasonable and customary charges allowed by the plan.
Amounts charged over the reasonable and customary do not count toward annual deductibles and out-of-pocket
maximums.
Be sure you understand the amount you will be required to pay out of your own pocket if you seek care out-of-network.
Out-of-Pocket Maximum: When you meet the annual out-of-pocket maximum, the plan will pay the full cost of
covered expenses for the remainder of the benefit year. Covered expenses (e.g. deductible and co-insurance amounts)
apply towards the out-of-pocket maximum. Prescription drug co-payments are NOT applied toward the out-of-pocket
maximum. In addition, out-of-pocket costs incurred for non-covered services or supplies in excess of the plan’s covered
expenses (e.g., expenses incurred for out-of-network services that exceed the reasonable and customary charges
allowed by the plan) are NOT applied toward the out-of-pocket maximum; these non-covered charges are the plan
participant’s financial responsibility.

12 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Milwaukee County Choice Plus Plan (PPO Comparable)
Not Participating
in Wellness Program
Participating
in Wellness Program
Employee Only $63.69 $44.77
Employee + Child/Children $89.08 $66.00
Employee + Spouse $127.38 $104.31
Employee + Family $140.31 $117.23
Milwaukee County Choice Plus Plan (PPO Comparable)
Not Participating
in Wellness Program
Participating
in Wellness Program
Employee Only $64.62 $45.69
Employee + Child/Children $76.62 $53.54
Employee + Spouse $107.77 $84.69
Employee + Family $120.00 $96.92
Milwaukee County Choice Plus Plan (PPO Comparable)
Not Participating
in Wellness Program
Participating
in Wellness Program
Employee Only $67.85 $47.49
Employee + Child/Children $80.54 $57.46
Employee + Spouse $113.08 $90.00
Employee + Family $126.00 $102.92
Employee Bi-Weekly Medical Premium Contributions
EFFECTIVE JANUARY 1, 2020
All Employees (except Deputy Sheriffs & Firefighters)
Deputy Sheriffs
Firefighters

Milwaukee County 2020 Benefits | 13
TOTAL REWARDS
Milwaukee County 2020 Benefits | 13

14 | Milwaukee County 2020 Benefits
TOTAL REWARDS
14 | Milwaukee County 2020 Benefits
When you don’t feel well, or your child is sick, the last thing you want
to do is leave the comfort of home to sit in a waiting room. Now, you
don’t have to.
A virtual visit lets you see and talk to a doctor from your mobile device
or computer without an appointment. Most visits take about 10 to 15
minutes and doctors can write a prescription*, if needed, that you can pick
up at your local pharmacy. And, it’s part of your health benets.
Conditions commonly treated through a virtual visit
Doctors can diagnose and treat a wide range of non-emergency
medical conditions, including:
To learn more, login to myuhc.com
• Bladder infection/
Urinary tract infection
• Bronchitis
• Cold/u
• Diarrhea
• Fever
• Migraine/headaches
• Pink eye
• Rash
• Sinus problems
• Sore throat
• Stomachache
Access virtual visits
Log in to myuhc.com
®
and choose from provider sites where you can
register for a virtual visit. After registering and requesting a visit you will pay
the $10.00 copay, and then you will enter a virtual waiting room. During
your visit you will be able to talk to a doctor about your health concerns,
symptoms and treatment options.
Get access to care online.
Anywhere. Any time.
• Anything requiring an exam or test
• Complex or chronic conditions
• Injuries requiring bandaging or
sprains/ broken bones
• Your doctor is not available
• You become ill while traveling
• You are considering visiting a
hospital emergency room for a
non-emergency health condition
Use virtual visits when:
Not good for:

Milwaukee County 2020 Benefits | 15
TOTAL REWARDS
16
Milwaukee County 2020 Benefits | 15

16 | Milwaukee County 2020 Benefits
TOTAL REWARDS
17
16 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 17
TOTAL REWARDS
2020 Dental Plan Coverage At-A-Glance
Delta Dental PPO or Premier
When you see a Delta Dental
PPO or Premier dentist
Noncontracted
When you see
a noncontracted dentist
Individual Annual Maximum
$3,000 $1,000 per person
individual
$25 $50
family
$75 $150
Dependent Eligibility
Dependents are eligible through the end of the month
in which they attain age 27
DIAGNOSTIC & PREVENTIVE SERVICES
Exams
100% 80%
Cleanings
100% 80%
Fluoride Treatments
100% 80%
X-rays
100% 80%
Sealants
100% 80%
Space Maintainers
100% 80%
Deductible applies?
No No
BASIC & MAJOR SERVICES
Emergency Treatments to Relieve Pain
100% 70%
Fillings
100% 70%
Endodontics — Nonsurgical
100% 70%
Endodontics — Surgical
100% 70%
Periodontics — Nonsurgical
100% 70%
Periodontics — Surgical
100% 70%
Extractions — Nonsurgical
100% 70%
Extractions — Surgical & Other Oral Surgery
100% 70%
Crowns, Inlays, Onlays
80% 50%
Bridges & Dentures
80% 50%
Repairs & Adjustments to Bridges & Dentures
80% 50%
Implants
80% 50%
Deductible applies?
Yes Yes
The summary below does not cover all plan details. Further information can be found in the summary plan description
or dental benefit handbook. That document provides a thorough explanation of your dental plan, including any
limitations or exclusions that might apply. If there are any discrepancies between information found here and the group
contract, the group contract shall govern.
Deductible
CONTINUED
2020 Dental Insurance
ADMINISTERED BY DELTA DENTAL

18 | Milwaukee County 2020 Benefits
TOTAL REWARDS
ORTHODONTIC SERVICES
Coverage Copayment
75% 0%
Individual Lifetime Maximum
$5,000 0
Deductible applies?
Yes
SPECIAL PLAN PROVISIONS
Evidence-Based Integrated Care Plan
Yes Yes
Check Up Plus
Yes Yes
Conventional Dental Plan (Delta Dental)
Employee Only $11.54
Employee + Child/Children $23.08
Employee + Spouse $23.08
Employee + Family $23.08
Conventional Dental Plan (Delta Dental)
Employee Only $5.54
Employee + Child/Children $9.23
Employee + Spouse $9.23
Employee + Family $9.23
Conventional Dental Plan (Delta Dental)
Employee Only $6.92
Employee + Child/Children $16.15
Employee + Spouse $16.15
Employee + Family $16.15
Employee Bi-Weekly Dental Premium Contributions
EFFECTIVE JANUARY 1, 2020
All Employees (except Deputy Sheriffs & Firefighters)
Deputy Sheriffs
Firefighters
2020 Dental Plan Coverage At-A-Glance
CONTINUED FROM PREVIOUS PAGE

Milwaukee County 2020 Benefits | 19
TOTAL REWARDS
Both networks provide you with the following:
Delta Dental oers two dental networks: Delta Dental
PPO
SM
and Delta Dental Premier®. Both save you
money. Dentists who belong to the Delta Dental PPO
network oer the lowest agreed-upon fees. And
the Delta Dental PPO network has more locations for
members to access care than any other PPO network.
Dentists who belong to the Delta Dental Premier
network also agree to discounts – just not as deep.
But the network is much broader; more than 81
percent of dentists nationwide belong to the Delta
Dental Premier network. The Delta Dental Premier
network is the nation’s largest dentist network.
See if your dentist belongs by visiting
www.deltadentalwi.com and clicking on
“Provider Search,” then “Find A Network Dentist.”
Treatment guarantees
Dentists agree to repair or replace
dental restorations should they fail
within 24 months.
No balance-billing
Dentists agree to a maximum fee –
if their normal charge is higher than
the maximum fee, they can’t pass
the balance on to you.
Claims processing
Dentists file claims on your
behalf. Payments go directly to the
dentist. No work for you!
How Delta Dental Provides You Value
Access broader networks. Save more money.
Estimated
Charge
Maximum
Allowed
Fees
Percentage
Paid by
Delta Dental
Amount
Delta Dental
Pays
Amount
Dentist can
Balance Bill
Total
Amount
You Pay
Your
Total Cost
Savings
Delta Dental
PPO
Network
$
1,200
$
825 80%
$
660
$
0
$
165
$
375
Delta Dental
Premier
Network
$
1,200
$
985 80%
$
788
$
0
$
197
$
215
Out-of-
Network
$
1,200
$
925 50%
$
462.50
$
275
$
737.50
$
0
Example Savings for a Common Procedure
Your
Total Cost
Savings
$
375
$
215
$
0
20
A
Delta Dental makes it for you to log on,
find the information you and get
on with your day.
the services
Access extensive dental benefits and utilization
Check
Request electronic EOBs
copays and
Review claim
Print ID
you in
20
A
Delta Dental makes it for you to log on,
find the information you and get
on with your day.
the services
Access extensive dental benefits and utilization
Check
Request electronic EOBs
copays and
Review claim
Print ID
you in
Milwaukee County 2020 Benefits | 19

20 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Network Benefit/Select Network Non-Network Reimbursement
Frequency —
Exams/Lenses or Contacts/Frames
12/12/24 months
Frequency based on date of service, not benefit plan year
Comprehensive Eye Exam
(one every 12 months)
Member pays $10, plan pays balance $40
Contact Lens Fit & Follow-Up
Standard — Lenses that are spherical power only,
soft lens materials, including planned replacement and
conventional lenses. Lenses are to be used in a daily
wear (removed prior to sleep) mode only
Member pays up to $40 $0
Contact Lens Fit & Follow-Up
Premium — Includes all lens powers and designs
other than spherical powers (e.g., toric, multifocal, etc.),
modes of wear that are extended or overnight schedules
and rigid or gas permeable materials
10% discount off retail $0
Laser Vision Correction
Lasik or PRK
15% off retail price
or 5% off promotional price
none
GLASSES
Frames
any available frame at provider location
(one every 24 months)
$125 allowance, then 20% off balance $90
Standard Plastic Lenses:
(one every 12 months)
Single Vision
Bifocal
Trifocal
Member pays $25, plan pays balance
$30
$50
$70
UV Coating
Member pays $15 none
Tint
(solid or gradient)
Member pays $15 none
Standard Scratch Resistance
Member pays $15 none
The DeltaVision benefit plan is administered through EyeMed Vision Care, one of the nation’s leading vision providers.
The plan includes coverage for important preventive eye care and discounts on laser vision correction.
The benefit summary below does not cover all plan details. Further information can be found in the Summary of
Benefits within the DeltaVision Benefit Handbook. That document provides a thorough explanation of your vision plan,
including any limitations or exclusions that might apply. If there are any discrepancies between information found here
and the group contract, the group contract shall govern.
Accessing Your DeltaVision Benefit
Receiving your vision benefit is as easy as visiting your nearest EyeMed Vision Care network provider. Inform your
provider you are a DeltaVision member with EyeMed and give them your full name and date of birth. You may present
your ID card, but it is not required to receive services.
2020 Vision Benefit
DELTAVISION BENEFIT PLAN ADMINISTERED THROUGH EYEMED VISION CARE
2020 Vision Benefit Coverage At-A-Glance
CONTINUED

Milwaukee County 2020 Benefits | 21
TOTAL REWARDS
All Employees (except Deputy Sheriffs)
DeltaVision
Employee Only $0.94
Employee + Child/Children $1.92
Employee + Spouse $1.88
Employee + Family $2.86
Dependent Age Limitation — dependents covered to age 26
Additional In-Network Discounts
• 20% discount on items not covered by the plan at network providers. This discount may
not be combined with any other discounts or promotional offers. This discount does not
apply to an Eye Med
®
provider’s professional services (e.g. exams) or contact lenses.
Retail prices may vary by location.
• 40% discount on complete eyeglass purchases after your plan benefits have been fully
used (includes prescription sunglasses).
• 15% discount on conventionaI contact lenses after your plan benefits have been fully used.
• Members can purchase eyeglasses online and apply their in-network eyeglass benefits
at www.glasses.com.
• Members can purchase contact lenses online and apply their in-network contact lenses
benefits at www.contactsdirect.com.
• Discounts do not apply for benefits provided by other group benefit plans.
How to Maximize Your DeltaVision Plan
• Use providers participating in your vision plan network; your benefit dollars will go
further at participating providers. For an up-to-date listing of EyeMed providers in your
area, visit www.deltadentalwi.com/visionproviders or call EyeMed’s Customer Care
Center at 844-848-7090.
• Use your full benefit allowance. Frames and lenses (plastic or contact) each have an
annual benefit allowance; the benefit allowance must be used on a single purchase day.
• Frequency of benefits: your benefit frequency is based on the date of service. For
example, you’ll be covered for another eye exam 12 months after your last eye exam.
• Participating providers may offer promotional pricing on vision materiaIs. You can
partake in either the DeltaVision Network Benefit or the promotional price available, but
not both. Your provider can help you to determine which is best for you. If you select the
promotional pricing you can submit your expenses for Non-Network Reimbursement.
• Prescription sunglasses can be purchased with your benefit allowance for frames and
plastic lenses.
• A 20% discount may be available on selected brands of non-prescription sunglasses
from participating providers. Ask your vision provider.
• Your vision benefits include both a frame allowance and a lens allowance. The lens
allowance will cover either eyeglass lenses or contact lenses. If you purchase both
glasses and contacts, you will be responsible for the cost of either the eyeglass lens or
the contacts, depending upon which was purchased first. Your provider can assist you
with making the best choice to maximize your vision benefit.
• Premium progressive lenses are more costly than standard progressive lenses. Please
discuss your costs for progressive lenses with your vision provider.
Plan Limitations/Exclusions
• Allowances are one-time use benefits; there is no remaining balance if entire allowance
is not used after initial purchase.
• Orthoptic or vision training, subnormal vision aids, and associated supplemental testing.
• Medical and/or surgical treatment of the eye, eyes or supporting structures.
• Corrective eyewear required by an employer as a condition of employment, and safety
eyewear unless specifically covered under the plan.
• Services provided as a result of any worker’s compensation law.
• Plano nonprescription lenses and nonprescription sunglasses (except for 20% discount).
• Aniseikonic lenses.
• Services or materials provided by any other group benefit providing vision care.
• Two pairs of glasses in lieu of bifocals.
• Lost or broken materials are not covered.
2020 Vision Coverage At-A-Glance
CONTINUED FROM PREVIOUS PAGE
Network Benefit/Select Network Non-Network Reimbursement
Standard Polycarbonate
Member pays $40 none
Standard Progressive
(add-on to bifocal)
Member pays $90, plan pays balance none
Standard Anti-Reflective Coating
Member pays $45 none
Other Add-Ons & Services
20% off retail price none
CONTACT LENSES
(In lieu of eyeglass lenses; one every 12 months. Contact lens allowance covers materials only.
Conventional
$150 allowance, then 15% off balance $150
Disposable
$150 allowance $150
Medically Necessary
Paid in full $210
Employee Bi-Weekly Vision Premium Contributions
EFFECTIVE JANUARY 1, 2020

22 | Milwaukee County 2020 Benefits
TOTAL REWARDS
There are two types of Flexible Spending Accounts (FSA). The first is a Health Care Flexible Spending Account and the
second is a Dependent Care Flexible Spending Account. The plan year for the Health Care Flexible Spending Account
runs from January 1 through March 15 of the following year and the Dependent Care Flexible Spending Account runs
from January 1 through December 31.
Your participation in a FSA plan allows a portion of your salary to be redirected to provide reimbursement for these
types of expenses.
• Health Care: To be eligible for reimbursement, the expense must be incurred for medical, dental, vision or
pharmacy care that is not reimbursed from any other source.
• Dependent Care: Work-related day care expenses for a qualifying dependent.
At the beginning of each plan year, you elect a specific dollar amount for each FSA you wish to participate in.
• Health Care: $2,750 maximum.
• Dependent Care: $2,500 maximum if “married, filing separately” or $5,000 maximum if single or “married, and
filing jointly.”
Participation in one or both FSAs can save you money by reducing your taxable income because taxes will be calculated
after the elected amount is deducted from your salary.
Your taxable income will also be reduced for Social Security calculation; therefore, there may be a corresponding
reduction in Social Security benefits.
“Use It or Lose It” Rule
Money remaining in your FSA account(s) will not be returned to you at the end of the plan year. Any amount remaining
after the end of the plan year will be forfeited. Because of the “use it or lose it” rule, it is important for you to carefully
estimate your out-of-pocket expenses for the upcoming plan year.
Flexible Spending Accounts
MILWAUKEE COUNTY EMPLOYER CONTRIBUTION TO FSA
Per the 2020 adopted budget, all employees, except those employees not contributing to ERS, who elect to
contribute their own funds into the Health Care Flexible Spending Account (FSA) will receive a dollar-for-dollar
matching contribution up to a maximum of $1,000 into their FSA plan from Milwaukee County.

Milwaukee County 2020 Benefits | 23
TOTAL REWARDS
What is a Health Care Flexible Spending
Account (FSA)?
A Health Care Flexible Spending Account (FSA) is an
employer-sponsored benefit that enables you to pay for
eligible expenses on a pre-tax basis. Any contributions
you make to your FSA are deducted from your check
before any of your taxes are calculated, reducing the
amount of your income that is taxed. Eligible employees
also receive a contribution to the FSA paid by Milwaukee
County.
The Health Care FSA can be used to reimburse you for
out-of-pocket medical, dental, vision or other health care
expenses.
How to Use Your FSA
Think of your flexible spending account as your own
personal bank account that you can use periodically to
reimburse yourself for qualified expenses. Each plan
year, the total amount you designate from your paycheck
and/or the Milwaukee County contribution is deposited
into your account.
Claims for eligible expenses that are not covered by a health care plan can be submitted directly to the FSA for
reimbursement. When you incur an eligible expense, you can use the Benefits Card, or you can complete a claim form.
To complete a claim form, attach your itemized, third-party receipt or the insurance company’s Explanation of Benefits
and mail or fax the information to Employee Benefits Corporation.
Claim reimbursement is based on the date you receive services, not the date you pay the invoice or the date you are
billed, which must be within January 1, 2020, and March 15, 2021. With the FSA, you can be reimbursed your entire
claim up to your plan-year election, including your Milwaukee County contribution minus any previous claim, even if
that amount has not yet been deducted from your pay.
Do not send claim forms to the Benefits Office.
WHAT EXPENSES CANNOT BE
REIMBURSED THROUGH THE FSA?
This is a partial list of expenses that do not qualify:
• Cosmetic surgery, procedures and/or
medications.
• Dental bleaching.
• Hair restoration (procedures, drugs or
medications).
• Health club or gym memberships for general
health.
• Marriage and family counseling.
• Over-the-counter drugs, or medications that are
not prescribed by your physician.
• Weight loss programs for general health
or appearance.
• Mail order prescriptions from another country.
• Premiums you or your spouse pay for insurance
coverage.

24 | Milwaukee County 2020 Benefits
TOTAL REWARDS
The Benets Card
Debit your BESTex
SM
Plan FSA directly
instead of paying out-of-pocket.
With the BESTex
SM
Plan, you set aside money from your paycheck
and place it in a Health Care Flexible Spending Account (FSA) to pay for
certain medical expenses before taxes are taken from your pay.
You use the Employee Benets Corporaon Benets Card to pay for
those expenses instead of using cash. The card debits your Health Care
FSA and makes the BESTex Plan even more convenient to use.
How the Benets Card Works
The Benets Card debits your Health Care FSA when you use the card
to pay for eligible health care expenses. For example, if your total
Health Care FSA elecon is $1,000, the card can pay for up to $1,000
worth of eligible health care expenses.
© 2017 Employee Benets Corporaon 1014-20 09/17 Standard
Contents
How the Benefits Card Works 1
IRS Regulations that Dictate Benefits Card Use 2
How You Receive Your Benefits Card 2
New Plan Year, Same Benefits Card 2
Cut-off Dates for Using the Card 2
Using the Benefits Card to Pay for End-of-Year Expenses 3
Keeping Your Card Active When You Move 3
Documentation Requests 3
Benefits Card Deactivation 3
Terminating Employment and the Card 4
Contact Employee Benefits Corporation 4
Quick Tips for Using the Benefits Card 4
24 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 25
TOTAL REWARDS
2 The BESTex Plan | The Benets Card
IRS Regulaons that Dictate Benets Card Use
There are several IRS regulaons that dictate how the Benets Card
works. Taking some me today to understand the most important
rules will help you use your card in the most convenient ways during
the plan year.
Eligible Expenses
You can use your Benets Card to pay for the same services and eligible
health care expenses that qualify under the Health Care FSA instead of
paying out-of-pocket.
Where You Can Use Your Benets Card
When you enroll in a standard health FSA, you can use your Benets
Card at health care, dental, and vision provider oces, or at retailers
and pharmacies that automacally substanate the transacon (verify
your expense is eligible) at the point of sale.
You may also use your Benets Card to pay for eligible OTC items that
are not considered a drug or medicine, such as bandages, contact
lens soluon, heang pads, ice packs, etc. Your card can only be
used for OTC medicaon purchased with a doctor’s prescripon at a
health provider’s oce, or at a retail pharmacy or merchant where a
pharmacist assigns a prescripon number and scannable bar code.
Refer to the Health Care FSA Eligible Expenses List for details.
When you enroll in a limited health FSA, you can use your Benets
Card at dental and vision provider oces. Your card can only be
used for dental and vision OTC items purchased at a dental or vision
provider’s oce (a doctor’s prescripon is necessary for any OTC
medicaon).
Any other purchases from providers that are not dental or vision
oces, including eligible expenses from approved retailers and
pharmacies, must be submied as claims for reimbursement from your
limited health FSA.
What To Do With Benets Card Expense Documentaon
Save your Benets Card expense documentaon! If your purchase is not
substanated at the point of sale, you will receive a Documentaon
Request asking you to submit itemized expense documentaon. The
documentaon allows us to verify that you used the card to pay for an
eligible expense, as required by the IRS.
These are federal mandates and the IRS provides no excepons.
You cannot use your Benets Card to pay for an expense that is already
covered by another plan such as health insurance, dental insurance,
vision insurance or health reimbursement arrangement. Before you
pay a doctor’s bill or other such expense, check to be sure that another
plan won’t be covering that bill. You can use your card to pay for the
poron of the expense that isn’t covered.
How You Receive Your Benets Card
Your employer has made the Benets Card part of your Health Care
FSA. You elect the card by elecng the Health Care FSA or compleng a
special elecon form.
Once you enroll, the Benets Card is mailed directly to your home.
The envelope will contain your card, a cardholder agreement and an
informaon yer. Watch for it to arrive within 30 days aer your plan
start date.
New Plan Year, Same Benets Card
If your employer has signed up for the Health Care FSA and you’ve
used your card this year, your new Health Care FSA elecons will be
automacally available on your card at the beginning of your new plan
year. As long as your employer connues the Health Care FSA, you’ll
receive a new card 30 days prior to your card expiraon date.
Cut-O Dates for Using the Benets Card
Generally, you can only use your Benets Card to pay for expenses that
you incur throughout your plan year. You cannot use your Benets
Card for prior plan year expenses. To be reimbursed during your runout
period for prior plan year expenses, submit those expenses as claims
for reimbursement.
Remember to ask for and SAVE
itemized expense documentaon
when you use your Benets Card!
3 things you should understand before
you use your Benets Card:
1
You may be asked to document your Benets Card purchases by
providing itemized expense documentaon.
2
Do not submit documentation until it is requested. We’ll send you
a list of card transactions that were not substantiated at the point of
sale, which you return to us with a copy of your documentation.
3
You will be asked to and must repay the expense amount if you
make a purchase with the card and, upon request, cannot provide
itemized expense documentation for the expense for any reason.
Milwaukee County 2020 Benefits | 25

26 | Milwaukee County 2020 Benefits
TOTAL REWARDS
3 The BESTex Plan | The Benets Card
If your employer’s plan includes a grace period, which extends your
plan year by 2 months and 15 days, the cuto dates for using your
Benets Card are extended, allowing you to use your Benets Card to
pay for eligible expenses you incur from the very beginning of the plan
year through the enre grace period. Once your grace period ends, you
cannot use the Benets Card for prior plan year expenses.
During your grace period, you may have expenses eligible for
reimbursement from two plan years – the earlier plan year and the
newly started plan year. Consider how you use your Benets Card
for new plan year expenses during the grace period if you have not
yet submied all of your earlier plan year’s expenses. Payments
and reimbursements are processed in the order they are received,
and during the grace period, the Benets Card applies all of your
transacons against the earlier plan year balance. Submit expenses
from the earlier plan year rst before subming any current plan year
expenses to ensure you receive your maximum benet payout.
Note: Please consult My Company Plan for the specic details dening
your company’s plan design.
When Your Expense Exceeds Your Available Balance
If your total eligible expense exceeds your Health Care FSA available
balance, you can use your Benets Card to pay for the amount
remaining in your account, and pay for the rest of the expense with
some other payment method.
To check your available balance, access your account at www.ebcflex.com
or contact us.
Keeping Your Card Acve When Your Address
or Name Changes
Be sure to update your address with your employer and with Employee
Benets Corporaon when you move or your card will be declined
at any merchant that uses an address vericaon process. Address
changes can be made online through My Account Assistant.
You should also be sure to update your employer and Employee Benefits
Corporation if you have a name change. Changes to your last name will result
in a new card being issued to you and a fee paid from your Health Care FSA.
Documentaon Requests
Your Benets Card tries to electronically verify your purchase is eligible
for payment from your Health Care FSA at the point of sale.
Many retailers and pharmacies automacally substanate the purchase
at the point of sale using an inventory informaon approval system
(IIAS). The IIAS determines whether expenses are eligible for payment
from the Health Care FSA and only pays for those expenses with the
Benets Card. Your receipt from these retailers and pharmacies oen
denote eligible expenses.
If the provider cannot substanate (automacally verify your expense is
eligible) at the me of payment, one of the following happens.
• Your card will be accepted and you will receive a Documentaon
Request to verify the expense is eligible for payment from your
Health Care FSA. We are required to request documentaon to verify
the enre expense is eligible.
-or-
• Your card will be declined. If you believe the purchase is eligible for
reimbursement from your Health Care FSA, you can pay for the
expense with another payment method and submit a claim for
reimbursement.
Receiving Documentaon Requests via Email
If you acvated your account at our website (www.ebcex.com) and
currently view your account online, we have the email address you
provided at that me. This is the email address we will use unless you
change it using My Account Assistant or contact us and request that we
change it. Log in to update your email preferences.
Benets Card Deacvaon
Deacvaon usually occurs because of outstanding, unsubstanated
expenses made using the card. You can request any outstanding
Documentaon Request. If you cannot supply valid, itemized expense
documentaon, you must repay the plan.
If your card privileges have been deacvated and your employer
renews your plan, your card will not be reinstated unl you send in valid
documentaon for the outstanding expenses or repay the plan.
26 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 27
TOTAL REWARDS
4 The BESTex Plan | The Benets Card
P: 800 346 2126
|
608 831 8445
F: 608 831 4790
P.O. Box 44347
Madison, WI 53744-4347
An employee-owned company
www.ebcex.com
Quick Tips for Using the Benets Card
The card may be declined for one of a few reasons:
1. The merchant does not accept the Benets Card.
See “IRS regulaons that dictate Benets Card use.”
2. The expense is not eligible under the Health Care FSA.
3. Your card has been temporarily suspended due to an
unsubstanated or ineligible expense.
You may have to submit expense documentaon for
transacons from some merchants, and not from others.
Many eligible merchants can automacally substanate – or
verify that the expenses paid for with the card are Health Care
FSA-eligible – your transacon at the point of sale, using an IIAS.
Others, including most health care providers, may not have this
capability.
You will receive Documentaon Requests by email if you have
an email address on le. These emails are not spam messages, so
be sure to watch for them. See “Documentaon Requests.”
Save your card, even aer you use up your Health Care FSA funds
or the BESTex Plan plan year ends. You will receive a new card 30
days prior to your card expiraon date. See “New plan year, same
Benets Card.”
Use the card to pay for out-of-pocket expenses eligible under your
plan. If you have a standard health FSA, this would include things
like prescripon and health plan co-payments, deducbles and
co-insurance; “Amount Due” on medical and dental statements;
orthodoncs; vision services and eyeglasses; eligible medical
supplies (bandages, ointments, rubbing alcohol, sunburn cream,
contact lens soluons/supplies, crutches, blood pressure and heart
rate monitors, and braces); and insulin & diabec supplies.
If you have a limited health FSA, this would include things like
dental or vision deducbles and co-insurance; “Amount Due” on
dental statements; orthodoncs; vision services and eyeglasses;
and eligible dental and vision supplies if purchased at a dental or
vision provider such as contact lens soluons/supplies.
Online and Mobile Benets Card Account Management
File claims, manage Benets
Card transacons, and upload
documentaon online or
using an Android or Apple
smartphone or tablet!
If a transacon needs
documentaon, you will
receive an email. Simply take a photo of your documentaon using
your mobile device’s camera, aach an image from the device’s
photo library or from your computer’s desktop and submit it to us.
Terminang Employment and the Card
Your Benets Card will be closed if you terminate employment with
the employer that oers the card. To submit claims during your run-out
period aer terminaon, you must use a Claim Form.
Contact Employee Benets Corporaon
If you have any quesons regarding the card or any aspect of your
BESTex Plan account, please email parcipantservices@ebcex.com
or contact the Parcipant Services Team at 800 346 2126.
Milwaukee County 2020 Benefits | 27

28 | Milwaukee County 2020 Benefits
TOTAL REWARDS
This worksheet will help you esmate the expenses for you, your spouse, and eligible dependents. Transfer the Deducon Per Pay Period for Health and Dependent Care FSAs
to the Enrollment Form.
Group Insurance Premiums
If you parcipate in your employer’s insurance plan(s), your premiums are deducted from your pay pre-tax unless you nofy your employer otherwise.
My BESTflex Plan Accounts
If you establish a Health Savings Account (HSA), you may enroll in the limited health FSA, which can only reimburse you for eligible dental, vision and preventave expenses and
the Dependent Care FSA. You can not contribute to your HSA in the same plan year that you parcipate in a standard health FSA.
My Plan Dates (Refer to “My Company Plan” Eligibility secon)
- - -
to
-
My Eecve Start Date (mm-dd-yyyy) My Plan Year Start (mm-yyyy) My Plan Year End (mm-yyyy) # Payroll Deducons
Examples of Eligible Health Care FSA Expenses:
This list is not meant to be all inclusive. Other
expenses not listed may also qualify. Please
refer to Secon 213 of the Internal Revenue
Code or call our toll free customer service line
800 346 2126.
DENTAL SERVICES
$_____ Crowns/Bridges
$_____ Dental X-Rays
$_____ Dentures
$_____ Exams/Teeth Cleanings
$_____ Extracons
$_____ Fillings
$_____ Gum Treatments
$_____ Oral Surgery
$_____ Orthodona/Braces
INSURANCE-RELATED ITEMS
$_____ Copays
$_____ Coinsurance
$_____ Deducbles
LAB EXAMS / TESTS
$_____ Blood Tests
$_____ Cardiographs
$_____ Diagnosc Fees
$_____ Laboratory Fees
$_____ Spinal Fluid Tests
$_____ Urine/Stool Analyses
$_____ X-Rays
MEDICATION
$_____ Insulin
$_____ Prescribed Birth Control
$_____ Prescribed Vitamins*
$_____ Prescripon Drugs (including
co-pays)*
VISION EXPENSES
$_____ Contact Lenses
$_____ Contact Lens Soluon & Cleaners
$_____ Eye Examinaons
$_____ Eyeglasses
$_____ Laser Eye Surgeries
$_____ Prescripon Sunglasses
$_____ Radial Keratotomy/LASIK
$_____ Reading Glasses
OTHER MEDICAL TREATMENTS/
PROCEDURES
$_____ Acupuncture
$_____ Alcoholism (inpaent treatment)
$_____ Chiropractor Services
$_____ Drug Addicon (inpaent treatment)
$_____ Hearing Exams
$_____ Hospital Services
$_____ Paerning Exercises
$_____ Physical Examinaon
(not employment related)
$_____ Physical Therapy
$_____ Speech Therapy
$_____ Sterilizaon
$_____ Vaccinaons and Immunizaons
$_____ Vasectomy and Vasectomy Reversals
$_____ Well Baby Care
OTHER MEDICAL SUPPLIES/SERVICES
$_____ Abdominal/Back Supports
$_____ Ambulance Services
$_____ Arch Supports/Orthoc Insoles
(requires doctor’s prescripon)
$_____ Blood Pressure Monitors
$_____ Breast Pumps & Lactaon Supplies
$_____ Compression Hosiery above
30 mmHg
$_____ Contracepves
$_____ Counseling (except for Marriage
and Family)
$_____ Crutches
$_____ Guide Dog (for visually/hearing
impaired person)
$_____ Hearing Aids & Baeries
$_____ Hospital Bed
$_____ Ice Pack
$_____ Insulin Supplies
$_____ Learning Disability
(special school/teacher)
$_____ Mastectomy Bras
$_____ Medic Alert Bracelet or Necklace
$_____ Medical Miles, Tolls, and Parking
$_____ Orthopedic Shoes**
$_____ Oxygen Equipment
$_____ Pregnancy Tests
$_____ Pre-Natal Vitamins
$_____ Prosthesis
$_____ Rubbing Alcohol
$_____ Splints/Casts
$_____ Sunscreen greater than SPF 14
$_____ Syringes
$_____ Transportaon Expenses
(essenal to medical care)
$_____ Wheelchair
$_____ Wigs (hair loss due to disease)
OVER-THE-COUNTER (OTC)
MEDICINE
Important note about OTC medicine
reimbursement: The Health Care FSA only
reimburses your OTC medicine expenses if
you have a doctor’s prescripon for them.
Doctor’s prescripons must include the
paent name, medicaon name, dosage,
me frame for treatment and any other
state law requirements. Only OTC drugs and
medicines with a prescripon and lled by the
pharmacy will be eligible for reimbursement.
Make sure you plan your annual Health Care
FSA elecon accordingly.
$_____ Allergy Medicines
$_____ Anhistamines
$_____ Analgesics
$_____ Antacids
$_____ An-Diarrhea Medicaons
$_____ An-Itch Medicaons
$_____ An-Nausea Medicaons
$_____ Aspirin
$_____ Athletes Foot Creams and Powders
$_____ Cold Sore Remedies
$_____ Cough Drops
$_____ Cough Syrups
$_____ Decongestants
$_____ Eye Drops
$_____ Fever Reducers
$_____ First Aid Cream (Bactine, special
diaper rash ointments, calamine lotion,
bug bite medication, wart remover
treatments)
$_____ Digesve Tract Relief Medicaons
$_____ Flu and Cold Medicaons
$_____ Hemorrhoidal Medicaons
$_____ Laxaves
$_____ Lice and Scabies Treatments
$_____ Menstrual Cycle Products
(for pain and cramp relief)
$_____ Moon Sickness Pills
$_____ Muscle / Joint Pain Relievers
$_____ Nasal Sinus Sprays
$_____ Nicone Gum / Patches
$_____ Pain Relievers
$_____ Pedialyte
$_____ Ren A (non-cosmec)
$_____ Rogaine***
$_____ Sinus Medicaons
$_____ Sleeping Aids
$_____ Smoking Cessaon Products
$_____ Sore Throat Sprays
$_____
Special Ointments / Cream for Sunburns
$_____ Throat Lozenges
$_____ Vapor Rubs
$_____ Weight Loss Drugs (only to treat a
specic disease)***
$_____ Yeast Infecon Treatments
* Excludes drugs imported from Canada and
other countries. Some medically necessary
items may be covered by the Health Care FSA if
prescribed by a physician for a specic medical
condion. The prescripon should contain the
specic medical condion and meframe for
treatment.
** Custom made shoes to treat or alleviate a
specic medical condion. Included with the
receipt should be a Leer of Medical Necessity
from a physician. The excess cost above the
normal cost of shoes is the eligible medical
expense.
*** Requires documentaon from the doctor or
care provider indicang use to treat a medical
condion. A Leer of Medical Necessity
template is available.
$___________________________________
Total Standard Health or Limited Health FSA
Elecon
$____________________________________
Divided by #Payrolls = Deduction per Pay Period
$____________________________________
Total Dependent Care FSA Elecon
$____________________________________
$_____________ Subtotal $_____________ Subtotal $_____________ Subtotal Divided by #Payrolls = Deduction per Pay Period
© 2017 Employee Benefits Corporation 117-17 10/17
Employee Worksheet
Fax to: 608 831 4790
Mail to: Employee Benets Corporaon, PO Box 44347, Madison WI 53744-4347
Phone support: 800 346 2126
|
608 831 8445
E-mail support: parcipantservices@ebcex.com
Employee Benefits Corporation
28 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 29
TOTAL REWARDS
Milwaukee County provides life insurance to help protect your family in the event of your death.
Basic Life Insurance
Milwaukee County Employees are eligible for up to 1 times their annual salary (on record as of the end of the previous
calendar year), rounded up to the next $1,000 in basic life insurance coverage. Milwaukee County provides the first
$25,000 ($20,000 for select bargaining units) of that coverage. If basic life is elected, employees are responsible for the
remainder of the coverage, at a rate of $0.47 per thousand dollars of covered income.
Example: Salary: $50,000 ››
The amount of your Basic Life Insurance on and after age 65 will be determined by applying the percentage from
the table below to the amount of your basic life insurance which would otherwise have been applicable had you not
become age 65:
Age Percentage
65 but younger than 66 92%
66 but younger than 67 84%
67 but younger than 68 76%
68 but younger than 69 68%
69 but younger than 70 60%
70 and older 25%
Enrollments after 30 days of employment will require evidence of insurability.
Additional Coverage
Employees may also elect additional life insurance coverage for themselves, their spouse, and dependent children.
Employee Optional Life Insurance
This optional life program offers seven different coverage choices in amounts from one times your annual salary up to
seven times your annual salary at favorable group rates.
The amount you select for optional life coverage will be in addition to your basic life election of one times your annual
salary of coverage.
If you meet the underwriting standards of MetLife* and are approved for coverage, premiums will be paid by you
through the convenience of bi-weekly payroll deduction. Optional life insurance is only available to active
employees and is not a retirement benefit.
The beneficiaries you designate for your basic life coverage will also apply to your optional life election.
Milwaukee County Life Insurance Plans
ADMINISTERED BY METLIFE
$50,000 – $25,000 = $25,000
$25,000 ÷ 1,000 = 25 x $0.47 = $11.75
$11.75 x 12 =
Cost: $141 annually / $5.52 biweekly

30 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Optional Life Insurance Premiums
To determine your bi-weekly premium, find the
appropriate rate in the table below (broken down by
age) and multiply it by the number of thousands of
dollars of insurance. Then, multiply it by 12 months
and divide by 26 pay periods to get the “per pay
period” deduction.
Enrollments after 30 days of employment will require
evidence of insurability and you will not be granted
the guarantee issue amount of $200,000.
Monthly Premium Rates
for Spouse Life Insurance
Spouse’s Age Rate per $1,000
younger than 30 $0.07
30–34 $0.09
35–39 $0.10
40–44 $0.13
45–49 $0.19
50–54 $0.33
55–59 $0.53
60–64 $0.92
65–70 $1.56
Monthly Premium Rates
Age Rate per $1,000
younger than 30 $0.08
30–34 $0.10
35–39 $0.12
40–44 $0.17
45–49 $0.25
50–54 $0.36
55–59 $0.57
60–64 $0.82
65–69 $1.27
70–74 $2.11
75 and older $3.69
Spouse Life Insurance
Your spouse life insurance benefit provides a benefit
to you and your family if your spouse should die while
you are an active employee of Milwaukee County.
The cost of this benefit is paid entirely by you on an
after-tax basis.
Employees may elect coverage for their spouse
in $10,000 increments. The maximum amount of
coverage is $250,000. To determine your bi-weekly
premium, find the appropriate rate in the table below
and multiply it by the number of thousands of dollars
of insurance. Then, multiply it by 12 months and
divide by 26 pay periods to get the “per pay period”
deduction.
In order for your dependent spouse to be covered for
spousal life insurance greater than $20,000, evidence
of insurability must be submitted to MetLife.
Enrollments after 30 days of employment will require
evidence of insurability, and you will not be granted the
guarantee issue amount of $20,000 for spouse life.

Milwaukee County 2020 Benefits | 31
TOTAL REWARDS
Dependent Child Life Insurance
Your dependent life insurance benefit provides a benefit to you and your family if your child(ren) should die while you
are an active employee of Milwaukee County. The cost for this benefit is paid entirely by you on an after-tax basis.
Employees may elect $5,000, $10,000, or $12,500 of coverage for their dependent children. The premiums for this
coverage are listed in the table below.
Coverage Amount Monthly
$5,000 $0.36
$10,000 $0.72
$12,500 $0.90
If you make a request during an annual open enrollment period, to increase your dependent life benefit to the next
higher level, evidence of insurability is not required. If you make a request to increase to more than the next higher
level of coverage, you must submit evidence of insurability for each of your dependents to MetLife.
“Dependent” for Purposes of Dependent Life Insurance means your unmarried child except for:
1. A person who is in the military or like forces of any country or of any subdivision of a country.
2. A person who is covered under this plan as an employee.
3. A person who lives outside the United States or Canada.
4. A child who:
a. Is 19 years of age or older and who is employed on a full-time basis.
b. Or, is 19 years of age or older and who is not a full-time student at an approved school.
c. Is 25 years of age or older.
If a dependent child is a covered person on the day before that child has reached the applicable age limit, that child
will continue to be a dependent after the age limit as long as:
a. That child is and remains unable to work in self-sustaining employment because of:
i. Physical handicap.
ii. Or, mental retardation.
b. And that child is and remains chiefly dependent upon you for support.
c. And that child is and remains a Dependent, as defined, except for the age limit.
d. And you give MetLife proof, when they ask for it, that the child is and remains so unable to work and
dependent upon you since the age limit. MetLife will not ask for proof more than once a year. The proof
must be satisfactory to MetLife.
Important Considerations
This is “term” insurance only. You may not borrow against it and no cash value accrues. You pay the bi-weekly premium
based on your age and coverage amount. Premiums will be deducted from all 26 paychecks.
Note: You may not apply for optional life coverage if you do not have “basic” coverage for any reason (for example, you
did not apply or want coverage when hired, or you voluntarily canceled coverage or lost coverage due to nonpayment of
premium while on leave of absence). You must first be approved for “basic” coverage through an insurability application.

32 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Auto and Home Milwaukee County Employees...
Make the most of your workplace benefits
with MetLife Auto & Home
®
Program description
MetLife Auto & Home’s group
insurance program is available
to you as a voluntary benefit
through your employer. This
program is underwritten by
MetLife Auto & Home and offers
special discounts to employees of
participating groups.
Maximize your company benefits today and start saving:
• Save up to an additional 10% right away with our Welcome Discount for NEW customers.
• Qualify for a group discount of up to 15% off your policy.
• Earn an additional discount when you pay your premium through automatic payroll deduction.
• Receive extra savings if you’ve been with your company for a long time.
• Save more with our superior driver discount.
• Earn multi-vehicle savings when you insure more than one vehicle with us.
• Make the most of our multi-policy discounts when you insure both your home and auto with MetLife Auto & Home.
Switch and save today!
Since everyone’s insurance policies renew at different times during the year, you may apply for group auto and home insurance at any time.
And coverage is 100% portable, so even if you change jobs you can take your policy with you. Take advantage of ALL your company benefits
and start saving today. Call 1 800 GET-MET 8 (1-800-438-6388) and see how MetLife Auto & Home makes it easier!
To make the most accurate comparisons, please have your current policies with you when you call, and provide your discount code: CZV
MetLife Auto & Home is a brand of Metropolitan Property and Casualty Insurance Company and its affiliates: Economy Fire & Casualty Company, Economy
Premier Assurance Company, Economy Preferred Insurance Company, Metropolitan Casualty Insurance Company, Metropolitan Direct Property and Casualty
Insurance Company, Metropolitan General Insurance Company, Metropolitan Group Property and Casualty Insurance Company, and Metropolitan Lloyds
Insurance Company of Texas, all with administrative home offices in Warwick, RI. Coverage, rates, discounts, and policy features vary by state and product, and
are available in most states to those who qualify. Met P&C
®
, MetCas
SM
, and MetGen
SM
are licensed in the state of Minnesota.
MetLife Auto & Home | 700 Quaker Lane | Warwick, RI 02887
1703 808079 1208-2982 1900031997(0418) L0418504283[exp0321][All States][DC] © 2018 MetLife Services and Solutions, LLC
32 | Milwaukee County 2020 Benefits
Milwaukee County 2020 Benefits | 33
TOTAL REWARDS
Protect yourself with affordable Hyatt Group Legal Services.
Legal matters, both planned and unplanned, are part of life. Enrolling in a Hyatt Legal Plan gives you the nancial and
emotional peace of mind to know you will be covered for expected and unexpected legal events.
The Hyatt Legal Plan provides you, your spouse and dependents with fully covered legal services from attorneys
experienced in estate planning documents, civil suits, adoption, identity theft issues and much more. Sign up for a
convenient payroll deduction of just $19.50 a month, and save hundreds over typical attorney fees... with no deductibles,
no co-pays, no claim forms or usage limits when using a Network Attorney. We’ll automatically deduct the cost from your
paychecks.
Choose from more than 14,000 attorneys nationwide.
Receive fully covered legal advice and representation for a wide range of legal matters. You can consult with your attorney
on the phone or in person. You can also use an out-of-network attorney and get reimbursed for covered services according
to a set fee schedule.*
It’s easy to access the right attorney. Online. By Phone. In Person.
Once you’re enrolled, simply go to members.legalplans.com or download our Mobile App. You can also call Hyatt Legal
Plans toll-free at 1-800-821-6400 Monday through Friday from 8 a.m. to 8 p.m. EST.
A representative will conrm your plan eligibility and give you a case number and the address and phone number of the
appropriate attorney(s) near you. Service is just a click or call away.
• Administrative Hearings
• Adoption
• Afdavits, Deeds
• Boundary or Title Disputes
• Civil Litigation Defense
• Consumer Protection
Matters
• Debt Collection Defense
• Demand Letters
• Divorce (20 hours)
• Document Review
• Domestic Violence
Protection
• Elder Law Matters
• Eviction and Tenant
Problems (for tenants)
• Guardianship
• Home Equity Loans
(primary, secondary or
vacation home)
• Identity Theft Defense
• Immigration Assistance
• Incompetency Defense
• Juvenile Court Defense
• **LifeStages - Identity
Management Services
• Living Wills
• Mortgages
• Name Change
• Personal Bankruptcy
• Personal Property Protection
• Powers of Attorney
• Prenuptial Agreement
• Promissory Notes
• Property Tax Assessment
• Restoration of Driving
Privileges
• Sale, Purchase or
Renancing (primary,
secondary or vacation home)
• Security Deposit Assistance
(for tenants)
• Small Claims Assistance
• Tax Audits
• Trafc Ticket Defense
(excludes DUI)
• **Triple Bureau Credit
Monitoring
• Trusts
• Wills, Codicils
• Zoning Applications
COVERED SERVICES
Questions? Call 1-800-821-6400
Monday–Friday 8:00 a.m.–8:00 p.m. (EST).
Peace of mind for you and your family.
Enrollment Period: December 4 - December 13, 2017
For more information and to Enroll, visit http://www.benetenroll.com
Live worry free.
*Exclusions and limitations apply. You will be responsible to pay the difference, if any, between the plan’s payment and the out-of-network attorney’s charge for services. Please see your plan description for complete details. **These benets provide the Participant with access
to LifeStages Identity Management Services and FraudScout Triple Bureau Credit Monitoring Services provided by CyberScout, LLC, formerly known as IDT911, LLC. CyberScout is not a corporate afliate of Hyatt Legal Plans. Group Legal Plans are provided by Hyatt Legal
Plans, Inc., a MetLife company, Cleveland, Ohio. In certain states, group legal plans are provided through insurance coverage underwritten by Metropolitan Property and Casualty Company and Afliates, Warwick, Rhode Island.
Milwaukee County 2020 Benefits | 33

34 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Using the internet to enroll is easy and
safe! Our secured website is set up to
take you automatically through each of
the following steps:
STEP 1 —
Log On to Main Menu
• The website will prompt you to enter
your User ID and your password.
• Your personal User ID is 1083+your
clock number.
• Your password is the first five digits of
your Social Security Number. This will
be your password unless you change it
using the “Change Password” option on
the home page.
• If your password does not work, call the Help Desk at (414) 278-7888. An operator will reset your password.
• From the main menu, select “New Hire Enrollment.”
STEP 2 — Check Your Demographic Information
• Is your address correct? If not, update your address in Ceridian Self Service.
• Enter your email address. If you forget your password, you can click “Forgot your password?” on the login screen
and a new one will be sent to your email address.
• If you have a maiden name you’d like to have on file, you may enter it here.
• Click Next to save your entries. If you “back” out, your entries will not be saved.
STEP 3 — Add / Update Your Dependents
• After reviewing your demographic information, the website will automatically take you to the “Dependent” screen.
Please provide your dependents’ information. You must ADD all dependents that you wish to cover in your benefit
plans. Click save after adding each dependent. Click “next” to confirm that your changes are accurate and continue.
STEP 4 — Enroll in Benefits
• Beginning with Medical coverage, select your medical plan. Once you have selected your plan, choose which level
of coverage you would like. The website will prompt you to repeat this election process for each benefit type. You
will only be shown benefits for which you are eligible.
STEP 5 — Review Your Confirmation Statement
• When you have completed your Benefit Enrollment, review your “Confirmation of Benefits” and be sure ALL
information is correct. If your intent is to cover dependents, check to be sure that each dependent is listed under
the benefit plan.
• If you need to change any information, simply click on the benefit link to go make changes to that benefit.
• You may print this document for your records.
Milwaukee County Benefit Enrollment System
Enroll Online
www.benefitenroll.com
6
Using the internet to enroll is easy and safe! Our secured website is set up to take you automatically through each of
the following steps:
STEP 1 Log On to Main Menu
The website will prompt you to enter your User ID and your Password.
Your personal User ID is 1083+your clock number.
Your Password is the first five digits of your Social Security Number. This will be your password unless you change it
using the “Change Password” option on the home page.
If your password does not work, call the Help Desk at 414-278-7888. An operator will reset your password.
From the main menu select New Hire Enrollment
STEP 2 Check your Demographic Information
Is your address correct? If not, update your address in Ceridian Self Service.
Enter your email address – if you forget your password, you can click “Forgot your password?” on the login screen and a
new one will be sent to your email address.
If you have a maiden name you’d like to have on file, you may enter it here.
Click Next to save your entries. If you “back” out, your entries will not be saved.
STEP 3 Register / Update Your Dependents
After reviewing your demographic information, the website will automatically take you to the “Dependent” screen.
Please provide your dependent/s’ information. You must ADD all dependents that you wish to cover in your benefit
plans. Click save after adding each dependent. Click next to confirm that your changes are accurate and continue.
STEP 4 Enroll In Benefits
Beginning with Medical coverage, select your medical plan. Once you have selected your plan, choose which level of
coverage you would like. The website will prompt you to repeat this election process for each benefit type. You will
only be shown benefits for which you are eligible.
STEP 5 Review Your Confirmation Statement
When you have completed your Benefit Enrollment, review your “Confirmation of Benefits” and be sure that ALL infor-
mation is correct. If your intent is to cover dependents, check to be sure that each dependent is listed under the bene-
fit plan.
If you need to change any information, simply click on the benefit link to go make changes to that benefit.
You may print this document for your records.
Questions? Need Help?
Call the Employee Benefits Division
414-278-4198
Milwaukee County – Benefit Enrollment
Enroll via the Internet at:
www.benefitenroll.com
QUESTIONS? NEED HELP?
Contact the Benefits Division
at (414) 278-4198.

Milwaukee County 2020 Benefits | 35
TOTAL REWARDS
7
How To Enroll – A Screen-By-Screen Guide
Upon logging in, Click on “New Hire Enrollment” or “Change Benefits”. You will be taken to the De-
mographic page. Check to make sure your information is correct. Enter an email address so if you
forget your password, one may be sent to you via email. Click “next”
to continue.
DEPENDENTS: You must first make sure your dependents are listed accurately, later you will
enroll them. Click the blue name to update a dependent. Click “add” to list a new dependent.
ELECTRONIC SIGNATURE: Accept this page to verify your truthfulness in enrolling.
MEDICAL: Select the medical election and level you wish. Click “next.” If you selected
“Employee + Child(ren)” and have more than one dependent, select which dependents you
are enrolling. Click “next” to continue.
7
How To Enroll – A Screen-By-Screen Guide
Upon logging in, Click on “New Hire Enrollment” or “Change Benefits”. You will be taken to the De-
mographic page. Check to make sure your information is correct. Enter an email address so if you
forget your password, one may be sent to you via email. Click “next”
to continue.
DEPENDENTS: You must first make sure your dependents are listed accurately, later you will
enroll them. Click the blue name to update a dependent. Click “add” to list a new dependent.
ELECTRONIC SIGNATURE: Accept this page to verify your truthfulness in enrolling.
MEDICAL: Select the medical election and level you wish. Click “next.” If you selected
“Employee + Child(ren)” and have more than one dependent, select which dependents you
are enrolling. Click “next” to continue.
LOG IN
Upon logging in, click on “New Hire Enrollment” or “Change Benefits.” You will be taken
to the Demographic page. Check to make sure your information is correct. Enter an email
address so if you forget your password, one may be sent to you via email.
Click “next” to continue.
DEPENDENTS
You must first make sure your dependents are listed accurately; later you will enroll them. Click the blue name to update a dependent.
Click “add” to list a new dependent.
ELECTRONIC SIGNATURE: Accept this page to attest to the accuracy of this information.
MEDICAL
Select the medical election and level you wish. Click “next.” If you selected “Employee + Child(ren)” and have more than one
dependent, select which dependents you are enrolling. Click “next” to continue.
HOW TO ENROLL ONLINE
A SCREEN-BY-SCREEN GUIDE
7
How To Enroll – A Screen-By-Screen Guide
Upon logging in, Click on “New Hire Enrollment” or “Change Benefits”. You will be taken to the De-
mographic page. Check to make sure your information is correct. Enter an email address so if you
forget your password, one may be sent to you via email. Click “next”
to continue.
DEPENDENTS: You must first make sure your dependents are listed accurately, later you will
enroll them. Click the blue name to update a dependent. Click “add” to list a new dependent.
ELECTRONIC SIGNATURE: Accept this page to verify your truthfulness in enrolling.
MEDICAL: Select the medical election and level you wish. Click “next.” If you selected
“Employee + Child(ren)” and have more than one dependent, select which dependents you
are enrolling. Click “next” to continue.
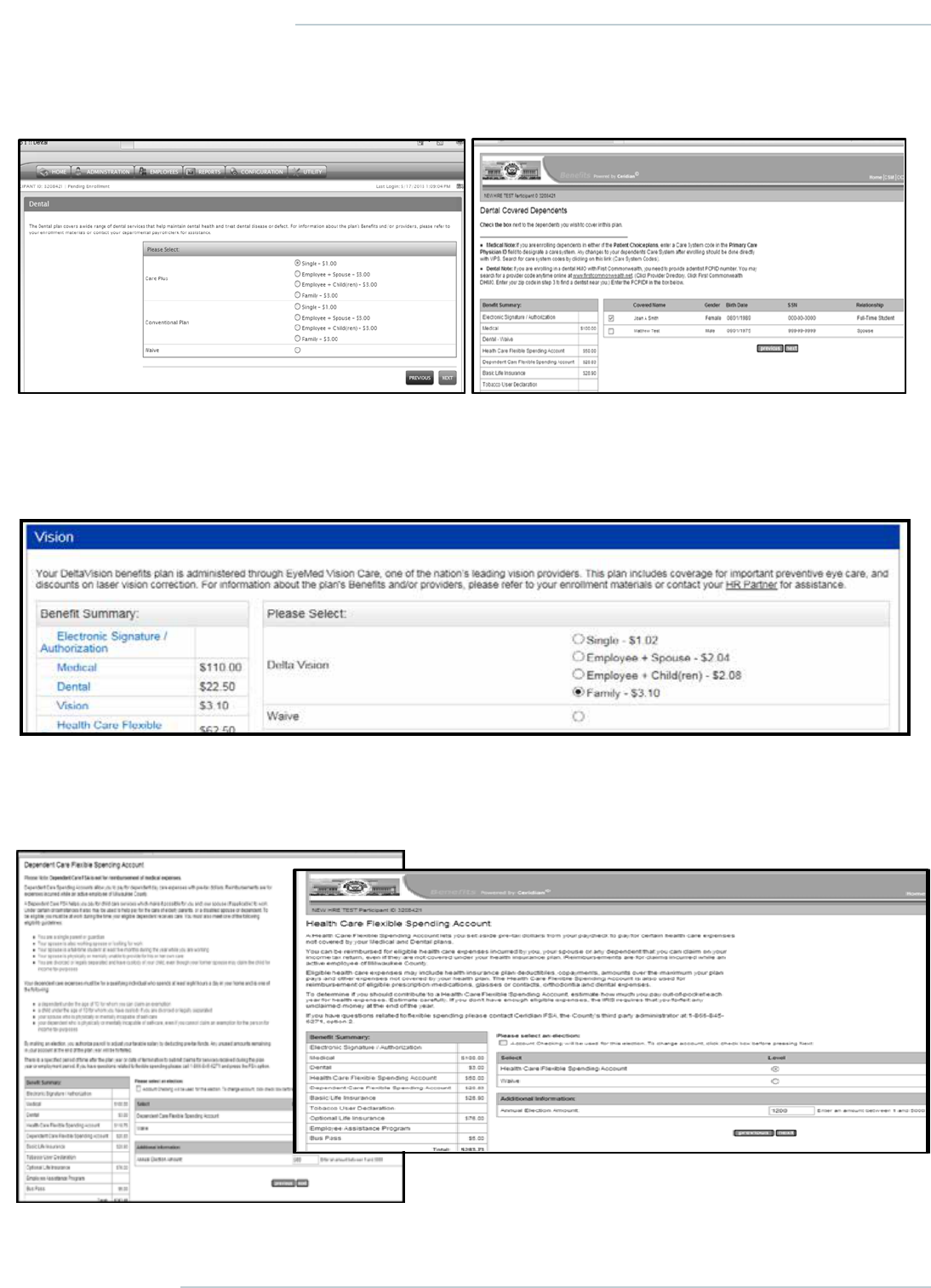
36 | Milwaukee County 2020 Benefits
TOTAL REWARDS
8
DENTAL: Select the dental election and level you wish. Click “next.” If you selected “family” and
have more than one dependent, select which dependents you are enrolling. Click “next” to contin-
ue.
FLEXIBLE SPENDING ACCOUNTS: You can put aside pre-tax dollars to pay for medical reim-
bursements with a Health Care FSA. You must enroll each year for this benefit.
A Dependent Care FSA may only be used for day
care expenses for your eligible dependent/s.
VISION: Select the level you wish. Click “next.” If you selected “Employee + Child(ren)” and
have more than one dependent, select which dependents you are enrolling. Click “next” to con-
tinue.
DENTAL
Select the level you wish. Click “next.” If you selected “family” and have more than one dependent, select which dependents you are
enrolling. Click “next” to continue.
VISION
Select the level you wish. Click “next.” If you selected “Employee + Child(ren)” and have more than one dependent, select which
dependents you are enrolling. Click “next” to continue.
FLEXIBLE SPENDING ACCOUNTS
You can set aside pre-tax dollars to pay for medical reimbursements with a Health Care FSA. You must enroll each year for this benefit.
A Dependent Care FSA may only be used for day care expenses
for your eligible dependent(s).

Milwaukee County 2020 Benefits | 37
TOTAL REWARDS
9
LIFE INSURANCE / BENEFICIARIES:
The county provides the option to enroll
in Basic Life Insurance. You must be en-
rolled in Basic Life to be able to enroll in
other types of Life Insurance. Basic life
insurance becomes effective 6 months
after enrollment.
OPTIONAL LIFE
Optional Life Insurance rates are based on
age.
You can choose how much life insurance
you want by clicking the button next to your
choice. Click “next” to continue.
SPOUSE LIFE INSURANCE
Spouse life insurance rates are based on age
Dependent Life Insurance
DEPENDENT LIFE
Employees can elect coverage for their depend-
ent children
9
LIFE INSURANCE / BENEFICIARIES:
The county provides the option to enroll
in Basic Life Insurance. You must be en-
rolled in Basic Life to be able to enroll in
other types of Life Insurance. Basic life
insurance becomes effective 6 months
after enrollment.
OPTIONAL LIFE
Optional Life Insurance rates are based on
age.
You can choose how much life insurance
you want by clicking the button next to your
choice. Click “next” to continue.
SPOUSE LIFE INSURANCE
Spouse life insurance rates are based on age
Dependent Life Insurance
DEPENDENT LIFE
Employees can elect coverage for their depend-
ent children
LIFE INSURANCE/BENEFICIARIES
The county provides the option to enroll in Basic Life
Insurance. You must be enrolled in Basic Life to be
able to enroll in other types of life insurance. Basic life
insurance becomes effective six months plus the first
day of the following month after your date of hire.
OPTIONAL LIFE
Optional Life Insurance rates are based on age.
You can choose how many times your salary by clicking
the button next to your choice. Click “next” to continue.
SPOUSE LIFE INSURANCE
Spouse life insurance rates are based on age.
DEPENDENT LIFE
Employees can elect coverage for their
dependent children.

38 | Milwaukee County 2020 Benefits
TOTAL REWARDS
10
OTHER BENEFITS:
Colonial Short Term Disability
and Empower Retirement
Deferred Compensation are
two benefits available to eligi-
ble employees. Employees
who wish to enroll in these
benefits need to enroll directly
with the carrier.
The Employee Assistance
Program is provided to all ac-
tive employees of Milwaukee
County. The EAP offers local
resources for financial planning
,
legal advice, relationship couns
el-
ing and many other programs f
or
managing life’s challenges.
Commuter Value Bus Pass --
All
Milwaukee County employees
are
eligible for a discounted Commuter Value
bus pass. Instructions for sign
ing up for
this benefit can be found on the
Bus Pass
enrollment screen.
These informational screens in the enrollment system
have instructions for contacting these carriers.
Confirmation of Benefits:
After completing the enrollment process, verify your
elections and dependent information.
If any section of your enrollment is incorrect or in-
complete, return to that section by clicking on the
name of the benefit. The system will return to the
Confirmation of Benefits screen after updates / cor-
rections have been made.
Click “save ” when you have finished reviewing your
elections. You will be returned to the home page.
Questions? Need Help?
Contact the Employee Benefits
Department at 414-278-4198
10
OTHER BENEFITS:
Colonial Short Term Disability
and Empower Retirement
Deferred Compensation are
two benefits available to eligi-
ble employees. Employees
who wish to enroll in these
benefits need to enroll directly
with the carrier.
The Employee Assistance
Program is provided to all ac-
tive employees of Milwaukee
County. The EAP offers local
resources for financial planning,
legal advice, relationship counsel-
ing and many other programs for
managing life’s challenges.
Commuter Value Bus Pass -- All
Milwaukee County employees are
eligible for a discounted Commuter Value
bus pass. Instructions for signing up for
this benefit can be found on the Bus Pass
enrollment screen.
These informational screens in the enrollment system
have instructions for contacting these carriers.
Confirmation of Benefits:
After completing the enrollment process, verify your
elections and dependent information.
If any section of your enrollment is incorrect or in-
complete, return to that section by clicking on the
name of the benefit. The system will return to the
Confirmation of Benefits screen after updates / cor-
rections have been made.
Click “save ” when you have finished reviewing your
elections. You will be returned to the home page.
Questions? Need Help?
Contact the Employee Benefits
Department at 414-278-4198
OTHER BENEFITS
Colonial Short Term Disability,
MetLife Home and Auto and
Empower Retirement Deferred
Compensation are three benefits
available to eligible employees.
Employees who wish to enroll in
these benefits need to enroll directly
with the carrier.
The Employee Assistance Program
is provided to all active employees of
Milwaukee County. The EAP offers local
resources for financial planning, legal
advice, relationship counseling and
many other programs for managing
life’s challenges.
All Milwaukee County employees are
eligible for a discounted Commuter
Value Bus Pass. Instructions for
signing up for this benefit can be found
on the Bus Pass enrollment screen.
The informational screens in the
enrollment system have instructions for
contacting these carriers.
CONFIRMATION OF BENEFITS
After completing the enrollment process, verify your elections and
dependent information.
If any section of your enrollment is incorrect or incomplete, return
to that section by clicking on the name of the benefit. The system
will return to the Confirmation of Benefits screen after updates/
corrections have been made.
Click “save” when you have finished reviewing your elections. You
will be returned to the home page.
QUESTIONS? NEED HELP?
Contact the Benefits Division
at (414) 278-4198.

Milwaukee County 2020 Benefits | 39
TOTAL REWARDS
48
Milwaukee County 2020 Benefits | 39

40 | Milwaukee County 2020 Benefits
TOTAL REWARDS
All active Milwaukee County Employees are eligible to
participate in the Commuter Value Pass (CVP) program
through the Milwaukee County Transit System (MCTS).
As a CVP participant, you will enjoy unlimited MCTS
transit, including Freeway Flyer and trolley service as
well as all special event shuttles (Summerfest, State
Fair, etc.) for only $10 per month (deducted equally over
26 pay periods)!
Enrollment Process
Employees must apply for the CVP program using the Benefit Enrollment System, print a copy of the enrollment
confirmation and bring it to the main transit office. Employees will have a photo taken and will be issued a bus pass on
site. The transit office is located at:
1942 North 17th Street
(Open Monday through Friday from 8 a.m. to 4 p.m.)
Enrollmentl will become effective on the first day of the following month.
Commuter Value Pass Program
QUESTIONS?
Call Milwaukee County Transit System at
(414) 343-1777 and ask about the CVP
for Milwaukee County, or contact the
Benefits Division at (414) 278-4198.

Milwaukee County 2020 Benefits | 41
TOTAL REWARDS
What is an Employee Assistance
Program (EAP)?
An EAP is a service designed to help you manage life’s
challenges. Everyone needs a helping hand once in a while,
and your EAP can provide it. EAP can refer you to professional
counselors and services that can help you resolve emotional
health, family and work issues. The following services, paid
for by Milwaukee County, are available.
Clinical Counseling
EAP can provide an assessment, assistance and referral to additional services when needed. Both face-to-face and
telephonic consultations are available. Eligible members are entitled to up to three counseling sessions per incident per
calendar year, for a wide range of emotional health issues, including:
• Marital, relationship, and family problems.
• Alcohol and drug dependency.
• Stress and anxiety.
• Depression.
• Grief and loss.
Work & Life Services
Telephonic consultations are available for:
• Financial issues and Federal tax assistance.
• Pre-retirement planning.
• Organizing life’s affairs.
• Concierge services.
• Legal services (telephonic or face-to-face).
Online Member Services
Access EAP information and tools online. With the click of a mouse you can:
• Search for an UnitedHealthcare counselor and get a referral.
• Manage your stress with interactive tools.
• Ask about an emotional health question.
• Obtain information on a wide variety of EAP-related topics.
Employee Assistance Program
ADMINISTERED BY UNITED BEHAVIORAL HEALTH
IF YOU NEED HELP
Call this toll-free number
24 hours/day, 7 days/week:
(800) 622-7276
or log on to www.liveandworkwell.com
access code: milwaukee

42 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Milwaukee County Human Resources
has partnered with Perkspot.com
to provide discounts to Milwaukee
County employees for a wide range of
retailers and service providers, including
electronics, clothing, vehicles, travel,
movie and sporting event tickets, and
many more. You can also request
Perkspot to negotiate new discounts
for Milwaukee County employees by
clicking on the “suggest a merchant”
feature at the top of the page. Discount
offers are updated frequently, and any
new discounts that either Perkspot or
Milwaukee County Human Resources
secures for County employees will be made available on the site.
To register, please visit mkecounty.perkspot.com. Registration is easy. All you need to provide is your zip code
and an e-mail address.
Employee Discount Program

Milwaukee County 2020 Benefits | 43
TOTAL REWARDS
Milwaukee County encourages all employees to seek out learning opportunities that enhance their skills and provide
career development. The Tuition Reimbursement Program was established to provide an opportunity for employees
to obtain additional education in order to increase their knowledge and abilities and prepare for future opportunities
within the County.
Eligibility
All benefit-eligible, regular appointment employees who are in good standing are eligible for this program upon
completion of one year of service to Milwaukee County. For the purpose of this program, an employee in good standing
is defined as an employee who at the time of submitting a pre-approval request has had no corrective action in the past
12 months, and who meets the performance expectations of his or her current position.
All other employees, including temporary, seasonal, hourly, interns and contract employees are ineligible.
Plan Reimbursement Level
Tuition reimbursement will be provided up to an annual maximum of $2,500 for employees with annual earnings less
than $75,000. Employees who earn $75,000 per year or more are limited to $1,500 per year. For this program, annual
earnings are defined as the employee’s base hourly pay rate multiplied by the full-time standard of 2,080 hours.
Overtime, bonuses, or other compensation will not be considered when applying this limit.
Reimbursement is limited to tuition only. Other expenses, such as textbooks and lab fees are not eligible.
The annual maximum is based on the calendar year, from January through December. Reimbursement will be applied
to the calendar year in which the class was successfully completed. For example, if a class is successfully completed
in December, but the reimbursement is not paid until January, the reimbursement is considered part of the prior year
annual maximum allowable amount.
Please see the full policy and request form on CountyConnect, the Milwaukee County intranet:
https://countyconnect.milwaukeecountywi.gov/MCINT/Human-Resources/Benefits/Tuition-Reimbursement.
Tuition Reimbursement Program

44 | Milwaukee County 2020 Benefits
TOTAL REWARDS
The Milwaukee County Health Matters Wellness Program is a voluntary benefit for
employees. We strive to improve the health of employees and their families.
All Milwaukee County employees are welcome to participate in the Health Matters
Wellness Program. If you are enrolled in the medical plan and choose to participate
in the program, you can earn a 30% reduction to your monthly insurance premium
contribution, up to a maximum of $50.
Participate in the following program activities:
• Online Health Questionnaire.
• Health Assessment/Population Health Risk Score (PHRS).
• Telephonic Health Coaching/Wellness Portal Challenges.
Online Health Questionnaire
Take a snapshot of your health! Login to the Wellness Portal and complete your 15-minute online health questionnaire.
Health Assessment/Population Health Risk Score (PHRS)
Gain insight to your health by completing your health assessment, which includes a biometric screening, obtaining
your Population Health Risk Score (PHRS) and health education session. Annual health assessments are conducted
in the first quarter (Q1) of the calendar year by Froedtert Workforce Health. Health Assessments take place over the
course of several weeks at all shift times and at a variety of Milwaukee County locations between January 6, 2020,
through March 5, 2020. Schedule your 30-mintue appointment on the Wellness Portal: www.workforcehealth.org/
mkecounty.
• Once you completed the health assessment and achieved a Population Health Risk score (PHRS) of 70 or higher,
you have earned a 30% reduction to your monthly insurance premium contribution, up to a maximum of $50.
• Once you completed the health assessment and achieved a Population Health Risk Score (PHRS) of 69 or below,
schedule a quarterly coaching session to continue earning the monthly insurance premium reduction. Visit the
Wellness Portal to complete telephonic health coaching sessions and/or wellness portal challenges quarterly to
continue to earn the monthly insurance premium reduction for 2020.
Your Population Health Risk Score (PHRS): Your PHRS is calculated by assigning a point value to each of your
health assessment test results. This helps to identify areas where you are doing well and areas that may need
improvement. Identifying these risk areas will help you to improve your overall health and well-being.
• Achieve a PHRS of 70 or higher: you have earned up to a 30% reduction to your monthly insurance premium
contribution up to a maximum of $50 for 2020.
• Achieve a PHRS of 69 or less: complete telephonic health coaching sessions and/or wellness portal challenges
quarterly to continue to earn the monthly insurance premium reduction for 2020.
Milwaukee County Wellness Program
Complete Online Questionnaire &
Health Assessment Between:
Begin Receiving Monthly
Insurance Reduction On:
Q1 January 2 to March 15, 2020 April 10, 2020
Q2 March 15 to June 15, 2020 July 17, 2020
Q3 June 15 to September 15, 2020 October 9, 2020
Q4 September 15 to November 30, 2020 December 18, 2020

Milwaukee County 2020 Benefits | 45
TOTAL REWARDS
Health Coaching/Wellness Portal Challenges
All employees are welcome to participate in a 15-minute telephonic health coaching session or complete a wellness
portal challenge. Visit the Wellness Portal to schedule your telephonic health coaching appointment or complete a
wellness portal challenge.
Biometric Verification Form
Have labs from your physician that include a fasting glucose test and lipid panel? Complete the Online Health
Questionnaire and submit your Biometric Verification Forms on the Wellness Portal during any of the quarter dates to
earn up to a 30% reduction to your monthly insurance premium contribution up to a maximum of $50 based on your
Population Health Risk Score (PHRS). (Note: If you submit Biometric Verification Forms, you do not need to attend a
Health Assessment session. Biometrics must be completed between January 2 and November 30, 2020.)
Pregnant Employees
Pregnant employees are welcome participate in the Health Matters Wellness Program. Complete the Online Health
Questionnaire and Pregnancy Waiver forms; submit forms on the Wellness Portal during any of the quarter dates and
earn up to a 30% reduction to your monthly insurance premium contribution up to a maximum of $50.
Newly Hired/Newly Eligible
New hires and staff who are newly eligible for benefits can participate in the Health Matters Wellness Program.
Within 60 days of hire or eligibility, complete the Online Health Questionnaire on the Wellness Portal at www.
workforcehealth.org/mkecounty and earn your 30% reduction to your monthly insurance premium contribution, up
to a maximum of $50.
To get started, access the Wellness Portal at www.workforcehealth.org/mkecounty.
New to the Wellness Portal? Follow these instructions to register:
1. Visit the wellness portal at www.workforcehealth.org/mkecounty.
2. Locate “New Users” box and click “Register.”
3. In the “New User Registration” box, please complete all fields. Company Code is 0045.
4. User ID is your 6-digit Clock Number.
5. Create and record your username and password to return to the Wellness Portal.
Returning user to the Wellness Portal?
Log into the Wellness Portal with the username and password you created.
Forgot username?
1. Click “Forgot Username” link on the Wellness Portal.
2. Enter company code: 0045 and User ID: 6-digit clock number.
You will receive an e-mail with the username you created (Note: The link expires after 30 minutes).
Forgot password?
1. Click “Forgot Password” on the Wellness Portal.
You will receive an e-mail with the username you created (Note: The link expires after 30 minutes).
If you still have troubles logging into the Wellness Portal, please contact Froedtert Workforce Health at 414-777-3446.

46 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Other Wellness Program Offerings for Milwaukee County Employees
There will be many opportunities to participate in wellness programs, separate from the annual health assessment.
These programs include:
Tobacco Cessation: We have resources to help you quit tobacco today! Visit the Wellness Portal to complete
the Quitting Smoking Action Plan, schedule a telephonic health coaching session and learn more about medication
available to you.
Blood Pressure Checks: Know your numbers and where you stand by being aware of your health. There are no
warning signs if you have high blood pressure. Regular checkups can help reduce your risk of developing high blood
pressure or any cardiovascular events such as a stroke or heart attack. Visit the Wellness Portal to view the schedule of
when and where you can get your blood pressure checked, for free!
HEALTH ASSESSMENT FREQUENTLY ASKED QUESTIONS
What is a health assessment?
A health assessment will give you a snapshot of your current health and help you identify your health-related risks. The
health assessment takes about 30 minutes and includes a biometric screening and health education session.
What is a biometric screening?
A biometric screening provides a clinical assessment of key health measures and may be used to identify certain health
conditions or areas of concern. A screening includes the following and is completed by healthcare professionals from
Froedtert Workforce Health.
• Blood pressure.
• Lipid profile (total cholesterol HDL, LDL, triglycerides).
• Blood glucose.
• Height, weight, waist circumference and body mass index (BMI).
• Nicotine use.
For accurate results, please fast (no food or liquids other than water; take medications as prescribed) for 8 hours before
your health assessment appointment.
Why should I participate in the annual health assessment process?
Approximately 70% of health conditions can be attributed directly to our lifestyle choices. Taking part in a health
assessment is a way to become aware of your current health status and help you identify areas that need improvement
for achieving optimal health.
By participating in the annual health assessment, you are able to:
• Measure your current health status and highlight any areas that need medical follow-up.
• Help you become aware of your health needs and lifestyle practices.
• Provide you with individualized feedback and guide you in achieving and maintaining good health.

Milwaukee County 2020 Benefits | 47
TOTAL REWARDS
What if I missed the annual health assessments at the beginning of the year?
If you have lab work from your physician dated January 2, 2020, or later, please submit your Biometric Verification Form
during Q2, Q3 or Q4 and begin earning your monthly insurance premium reduction based on your Population Health Risk
Score (PHRS).
What information will my employer receive?
Your employer will receive a summary report that provides a statistical picture of the health status of the company as
a whole. There are no names used in this report, only the total for the categories of questions (aggregate data). This
information will be used to plan appropriate wellness opportunities for the company.
Milwaukee County works with experts from Froedtert Workforce Health to administer the health assessments.
Froedtert Workforce Health must follow the same laws and regulations as your personal physician and will not share
your personal health information with Milwaukee County, its agencies, or any other organization. Froedtert Workforce
Health will only provide Milwaukee County with aggregate data and general population health reports for future
planning purposes. Your individual private health information cannot be determined from the aggregate data.
Will I be able to complete my health assessment during work time?
It is recommended to be done on work time, but please discuss this with your manager or supervisor.
IMPORTANT INFORMATION
• Spouses and dependents are not required to participate in order for the employee to receive the incentive.
• For accurate results, please fast (no food or liquids other than water; take medications as prescribed) for 8 hours
before your health assessment appointment.
• Health coaching is a one-on-one interaction with a certified health coach who is there to help you achieve your
health-related goals and keep you accountable.
• Communication with your health coach during your coaching session is confidential and not reported back to
Milwaukee County.
• If you think you might be unable to participate or meet a standard for a reward under this program, you may qualify
for an opportunity to earn the same reward by different means. Contact the Milwaukee County Wellness Coordinator
at (414) 278-4938 to find a program with the same reward that is right for you in light of your health status.
• The Workforce Health Wellness Portal is accessible from work or home on a desktop computer, tablet or
smartphone at www.workforcehealth.org/mkecounty.
CONTACT INFORMATION
Milwaukee County Wellness Coordinator: (414) 278-4938
Milwaukee County Benefits Division: (414) 278-4198
Froedtert Workforce Health: (414) 777-3446

48 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Mandatory Direct Deposit
Direct Deposit of payroll checks is mandatory for all Milwaukee County employees.
• Direct Deposit to Your Bank or Credit Union: Ceridian Self Service provides all the necessary tools to get you
started on direct deposit with your bank or credit union. Ask your payroll clerk what you need to do to begin the
direct deposit of your check.
• U.S. Bank Focus Debit Card: Employees who need another alternative to direct deposit should consider the
U. S. Bank Focus Card. The Focus Card does not require that you have a bank account, nor does it require any pre-
approval. The Focus Card is instead a debit card, where your net pay is deposited.
What is the Focus Card?
• A Visa prepaid card issued by U.S. Bank.
• Payroll is automatically loaded to the card just like
direct deposit to a bank.
• Works like other Visa debit cards to make purchases,
pay bills or get cash.
Why Use a Prepaid Card?
• Convenient: Allows employees to payroll
electronically without needing a bank.
• Fast: Funds available the morning of payroll.
No waiting for a check.
• Safe: Safer than carrying cash. Visa protection if lost or stolen.
• Ideal for employees who don’t have or want a bank or want a separate account to help with budgeting.
Using the Focus Card
• Use at millions of places that accept debit cards.
• Make purchases in stores, over the phone or online, or pay bills.
• Get cash at over 1.3 million Visa/Plus® ATMs.
• Use the cash-back option at participating merchants, such as grocery stores.
Go to Ceridian Self Service to sign up for a U.S. Bank Focus Card, or see your payroll clerk for more information. Fees
are minimal if card is lost or you exceed the card balance.
Mandatory Direct Deposit of Payroll Checks
44
Mandatory Direct Deposit of Payroll Checks
Mandatory Direct Deposit. Direct Deposit of payroll checks is mandatory for all Milwaukee
County Employees.
Direct Deposit to Your Bank or Credit Union:. Ceridian Self Service provides all the neces-
sary tools to get you started on direct deposit with your Bank, or Credit Union. Ask your payroll
clerk what you need to do to begin the direct deposit of your check.
U.S. Bank Focus Debit Card: Employees who need another alternative to direct deposit
should consider the U. S. Bank Focus Card. The Focus Card does not require that you have
a bank account, nor does it require any pre-approval. The Focus Card is instead a debit card,
where your net pay is
deposited.
What is the Focus Card?
A prepaid card issued by U.S.
Payroll is automatically loaded to the card just like direct
deposit to a bank
Works like other Visa debit cards to make
pay bills or get
a Card?
Convenient Allows employees to payroll electronically without needing a
bank
Fast Funds available the morning of payroll No waiting a
Safe Safer than carrying cash. Visa protection if lost or stolen
Ideal for employees
Don't have or want a bank
Want a separate account to help with
Using the Focus Card –
- Use at millions of places that accept debit cards
- Make purchases in stores, over the phone, online or pay bills
- Get cash at over 1.3 million Visa/Plus® ATMs.
- Use the cash-back option at participating merchants like grocery stores
Go to Ceridian Self Service to sign up for a U.S. Bank Focus Card or see your payroll clerk for
more information. Fees are minimal if card is lost or you exceed the card balance.

Milwaukee County 2020 Benefits | 49
TOTAL REWARDS
45
The Employees’ Retirement System (ERS) is a single-employer plan that was created to encourage
qualified personnel to enter and remain in the service of the County of Milwaukee by providing a sys-
tem of retirement, disability and death benefits to or on behalf of its employees. The County was
mandated to create the ERS as a separate legal entity with the passage of Chapter 201 of the Wis-
consin State Statues in 1937.
The authority to manage and administer the ERS is vested in the Pension Board. The Pension
Board consists of ten members – three members appointed by the County Executive (subject to con-
firmation by the County Board of Supervisors), two members appointed by the County Board Chair-
man (subject to confirmation of the County Board and County Executive), four elected members
consisting of three employee-members and one retired member, and one member appointed by the
Deputy Sheriff Association.
The County and ERS members make contributions to ERS based on actuarially determined contri-
bution requirements, as well as additional contributions made at the discretion of the County Board.
Actuarially determined contribution requirements are set during the County’s budget process.
Benefits
Participation in ERS is automatic with the exception of excluded employees (i.e., Pension Board and
Commission members and employees covered under the OBRA Plan). Benefits available include:
Monthly Pension Benefit
Disability Benefit
Death Benefit
The normal retirement benefit is a monthly pension for the life of the participant. For most employ-
ees, the formula used to determine the monthly pension benefit is based on a multiplier (the multipli-
er is determined by Ordinance, Union contract and ERS enrollment date) times service credits times
the final average salary. Service credits, in general, are based on the years of employment history
with the County. Final average salary for most members is a calculation based on the three highest
consecutive years of earnings. The formula includes various dates, union contracts, Milwaukee
County Ordinances, State Statutes and other qualifying factors.
To receive a pension benefit from Milwaukee County, you must satisfy age and vesting require-
ments. To receive a normal retirement pension you must be 55 with 30 service credits, age 60 and
vested or age 64 and vested. If you are at or beyond your normal retirement age when joining Mil-
waukee County, you are automatically vested. You could also be eligible for an early retirement
pension at age 55 with 15 service credits.
Retirement Benefits
The Employees’ Retirement System (ERS) is a single-employer plan that
was created to encourage qualified personnel to enter and remain in
the service of Milwaukee County by providing a system of retirement,
disability and death benefits to or on behalf of its employees. The County
was mandated to create the ERS as a separate legal entity with the
passage of Chapter 201 of the Wisconsin State Statues in 1937.
The authority to manage and administer the ERS is vested in the Pension
Board. The Pension Board consists of 10 members – three members
appointed by the County Executive (subject to confirmation by the County Board of Supervisors), two members
appointed by the County Board Chairman (subject to confirmation of the County Board and County Executive), four
elected members consisting of three employee-members and one retired member, and one member appointed by the
Deputy Sheriff Association.
The County and ERS members make contributions to ERS based on actuarially determined contribution requirements,
as well as additional contributions made at the discretion of the County Board. Actuarially determined contribution
requirements are set during the County’s budget process.
Benefits
Participation in ERS is automatic with the exception of excluded employees (i.e., Pension Board and Commission
members and employees covered under the OBRA Plan). Benefits available include:
• Monthly Pension Benefit.
• Disability Benefit.
• Death Benefit.
The normal retirement benefit is a monthly pension for the life of the participant. For most employees, the formula used
to determine the monthly pension benefit is based on a multiplier (the multiplier is determined by ordinance, union
contract and ERS enrollment date) times service credits times the final average salary. Service credits, in general, are
based on the years of employment history with the County. Final average salary for most members is a calculation
based on the three highest consecutive years of earnings. The formula includes various dates, union contracts,
Milwaukee County Ordinances, State Statutes and other qualifying factors.
To receive a pension benefit from Milwaukee County, you must satisfy age and vesting requirements. To receive a
normal retirement pension you must be 55 with 30 service credits, age 60 and vested or age 64 and vested. If you are
at or beyond your normal retirement age when joining Milwaukee County, you are automatically vested. You could also
be eligible for an early retirement pension at age 55 with 15 service credits.
If you leave Milwaukee County employment prior to attaining your normal retirement age and are vested, you may be
eligible to receive a deferred retirement pension when you reach your normal retirement age.
If you have service credit from one of the other public retirement systems (State of Wisconsin Retirement System or
City of Milwaukee Employees Retirement System), there may be special provisions available. This information should
be provided to ERS at the time of your employment.
Retirement Benefits

50 | Milwaukee County 2020 Benefits
TOTAL REWARDS
A member is considered vested to receive a pension benefit with:
• Five service credits.
• Military Service Credit (add-on).
• Reciprocity Service Credit (vesting and pension enhancement in other systems).
Deputy sheriffs are required to have 10 service credits for vesting.
For additional information regarding the Employees’ Retirement System, please call (414) 278-4207.

Milwaukee County 2020 Benefits | 51
TOTAL REWARDS
What is a deferred compensation plan?
The Milwaukee County Deferred Compensation Plan (Plan) is a governmental 457(b) deferred compensation plan that
allows employees to supplement any existing retirement and pension benefits by saving and investing traditional
before-tax dollars and/or ROTH after-tax dollars as 457(b) elective contributions.
Why should I participate in the Plan?
You may want to participate if you are interested in saving and investing additional money for retirement and/or in the
case of before-tax contributions, reducing the amount of current state and federal income tax you pay each year. Your
Milwaukee County Deferred Compensation Plan can be an excellent tool to help reach your retirement goals.
You may also qualify for federal income tax credit by participating in this Plan. For more information about this tax
credit, please contact the Milwaukee County 457 service center at (877) 457-6459 or (414) 223-1921.
1
Who is eligible to enroll?
All full-time, part-time, and hourly employees of Milwaukee County are immediately eligible to participate in the Plan.
Please contact the Milwaukee County 457 staff at (414) 223-1921 if you have any questions and to enroll in the Plan.
Individuals who have separated from service or have retired are eligible to keep their balance in the Plan.
What are the contribution limits?
In 2019, the maximum amount you may defer from your salary is 100% or your includible compensation (as defined by
the Internal Revenue Code) or $19,000, whichever is less. This is the total amount you may contribute with before- and
after-tax contributions combined.
Those participants who are age 50 and older may contribute an additional $6,000 to the Plan in 2019. This means that
participants age 50 and older can contribute a maximum or $25,000 or 100% or includible compensation, whichever is
less, for the 2019 calendar year.
For more information, you may contact the local office located in the Milwaukee County Courthouse, 901 North 9th
Street, Room 212C, or call (414) 223-1921 or (877) 457-6459.
Core securities, when offered, are offered through GWFS Equities, Inc. and/or other broker-dealers. Great-West Financial
®
, Empower Retirement
and Great-West Investments
™
are the marketing names of Great-West Life & Annuity Insurance Company, Corporate Headquarters: Greenwood Village, CO;
Great-West Life & Annuity Insurance Company of New York, Home Office: New York, NY, and their subsidiaries and affiliates, including registered investment
advisers Advised Assets Group, LLC and Great-West Capital Management, LLC. AM677133-1118
1
This material has been prepared for informational and educational purposes only and is not intended to provide
investment, legal or tax advice.
Milwaukee County’s Deferred Compensation Plan
ADMINISTERED BY EMPOWER RETIREMENT
51
Milwaukee County’s Deferred Compensation Plan
Administered by Empower Retirement
What is a Deferred Compensation Plan?
The Milwaukee County Deferred Compensation Plan (Plan) is a governmental 457(b) deferred compensation plan that
allows employees to supplement any existing retirement and pension benefits by saving and investing traditional
before-tax dollars and/or ROTH after-tax dollars as 457(b) elective contributions.
Why should I participate in the Plan?
You may want to participate if you are interested in saving and investing additional money for retirement and/or in the
case of before-tax contributions, reducing the amount of current state and federal income tax you pay each year. Your
Milwaukee County Deferred Compensation Plan can be an excellent tool to help reach your retirement goals.
You may also qualify for federal income tax credit by participating in this Plan. For more information about this tax
credit please contact the Milwaukee County 457 service center at (877) 457-6459 or (414) 223-1921.
1
Who is eligible to enroll?
All full time, part time, and hourly employees of Milwaukee County are immediately eligible to participate in the Plan.
Please contact the Milwaukee County 457 staff at (414) 223-1921 if you have any questions and to enroll in the Plan.
Individuals who have separated from service or have retired are eligible to keep their balance in the Plan.
What are the contribution limits?
In 2019, the maximum amount you may defer from your salary is 100% or your includible compensation (as defined by
the Internal Revenue Code) or $19,000, whichever is less. This is the total amount you may contribute with before- and
after-tax contributions combined.
Those participants who are age 50 and older may contribute an additional $6,000 to the Plan in 2019. This means that
participants age 50 and older can contribute a maximum of $25,000 or 100% of includible compensation, whichever is
less, for the 2019 calendar year.
For more information, you may contact the local office located in the Milwaukee County Courthouse, 901 N. 9
TH
Street,
Room 212C or by calling (414) 223-1921 or (877) 457-6459.
Core securities, when offered, are offered through GWFS Equities, Inc. and/or other broker-dealers. Great-West Financial
®
, Empower Retirement
and Great-West Investments™
are the marketing names of Great-West Life & Annuity Insurance Company, Corporate Headquarters: Greenwood
Village, CO; Great-West Life & Annuity Insurance Company of New York, Home Office: New York, NY, and their subsidiaries and affiliates, including
registered investment advisers Advised Assets Group, LLC and Great-West Capital Management, LLC.
AM677133-1118
1
This material has been prepared for informational and educational purposes only and is not intended to provide
investment, legal or tax advice.

52 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Important Notice From Milwaukee County About Your Prescription Drug Coverage
And Medicare...................................................................................................................................... 53
Notice to Enrollees In A Self-Funded Nonfederal Governmental Group Health Plan
For Plan Years Beginning On Or After September 23, 2010 ............................................................... 55
Women’s Health And Cancer Rights Act Notice ................................................................................ 56
Notice Of Coverage For Newborns And Mothers ............................................................................... 56
Notice Regarding Wellness Program .................................................................................................. 57
Protections From Disclosure Of Medical Information ........................................................................ 58
New Health Insurance Marketplace Coverage Options And Your Health Coverage ......................... 59
Premium Assistance Under Medicaid And The Children’s Health Insurance Program (CHIP) ........... 61
2020 Annual Notices
52 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 53
TOTAL REWARDS
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug
coverage with Milwaukee County and about your options under Medicare’s prescription drug coverage. This information can help you
decide whether or not you want to join a Medicare drug plan. Information about where you can get help to make decisions about your
prescription drug coverage is at the end of this notice.
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can
get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan
(like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least
a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher
monthly premium.
2. Willis of Wisconsin, Inc., on behalf of Milwaukee County, has determined that the prescription drug
coverage offered by Milwaukee County is, on average for all plan participants, expected to pay out as
much as standard Medicare prescription drug coverage pays and is considered Creditable Coverage.
Because the prescription drug coverage offered by Milwaukee County is, on average for all plan participants, expected
to pay out as much as standard Medicare prescription drug coverage pays, it is considered Creditable Coverage. It is
not necessary for you to join a Medicare prescription drug plan at this time.
Your existing coverage is, on average, at least as good as standard Medicare prescription drug coverage. You can keep
this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
You can join a Medicare drug plan when you first become eligible for Medicare and each year from November 15 through December
31. This may mean that you may have to wait to join a Medicare drug plan and that you may pay a higher premium (a penalty) if you
join later. You may pay that higher premium (a penalty) as long as you have Medicare prescription drug coverage. However, if you lose
creditable prescription drug coverage, through no fault of your own, you will be eligible for a sixty (60) day Special Enrollment Period
(SEP) because you lost creditable coverage to join a Part D plan. In addition, if you lose or decide to leave employer/union sponsored
coverage; you will be eligible to join a Part D plan at that time using an Employer Group Special Enrollment Period. You should
compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering
Medicare prescription drug coverage in your area.
If you decide to join a Medicare drug plan, your Milwaukee County coverage will not be affected. See below for more
information about what happens to your current coverage if you join a Medicare drug plan.
Your current coverage pays for other health expenses in addition to prescription drugs. If you enroll in a Medicare prescription drug
plan, you and your eligible dependents will still be eligible to receive all of your current health and prescription drug benefits and the
Medicare prescription drug plan will coordinate benefits with your Milwaukee County prescription drug coverage.
If you do decide to join a Medicare drug plan and drop your Milwaukee County coverage, be aware that you and your dependents may
not be able to get this coverage back.
You should also know that if you drop or lose your coverage with Milwaukee County and do not join a Medicare drug plan within 63
continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later.
Important Notice From Milwaukee County
About Your Prescription Drug Coverage And Medicare
2020 ANNUAL NOTICES
Milwaukee County 2020 Benefits | 53

54 | Milwaukee County 2020 Benefits
TOTAL REWARDS
If you go 63 continuous days or longer without prescription drug coverage that was at least as good as Medicare’s prescription drug
coverage, your monthly premium may go up by at least 1% of the base beneficiary premium per month for every month that you did
not have that coverage. For example, if you go 19 months without coverage, your premium may consistently be at least 19% higher
than the base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription
drug coverage. In addition, you may have to wait until the following November to join.
For more information about this notice or your current prescription drug coverage:
• Contact the person listed below for further information.
• Note: You will get this notice each year. You will also get this notice before the next period you can join a Medicare drug plan,
and/or if this coverage through Milwaukee County changes. You also may request a copy.
For more information about your options under Medicare prescription drug coverage:
• More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You
will get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans.
For more information about Medicare prescription drug coverage:
• Visit www.medicare.gov.
• Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook
for their telephone number) for personalized help.
• Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about
this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare Drug Plans, you may
be required to provide a copy of this notice when you join to show whether or not you have maintained creditable
coverage and whether or not you are required to pay a higher premium (a penalty).
Date: October 31, 2019
Name of Entity/Sender: Milwaukee County
Contact—Position/Office: Division of Employee Benefits
Address: 901 North 9th Street, Room 210; Milwaukee, WI 53233
Phone Number: (414) 278-4198
54 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 55
TOTAL REWARDS
Group health plans sponsored by State and local governmental employers must generally comply with Federal law requirements in
title XXVII of the Public Health Service Act. However, these employers are permitted to elect to exempt a plan from the requirements
listed below for any part of the plan that is “self-funded” by the employer, rather than provided through a health insurance policy.
Milwaukee County has elected to exempt Milwaukee County Choice Plus Plan from the following requirements:
1. Protection against limiting hospital stays in connection with the birth of a child to less than 48 hours for a vaginal
delivery, and 96 hours for a cesarean section.
2. Protections against having benefits for mental health and substance use disorders be subject to more restrictions
than apply to medical and surgical benefits covered by the plan.
3. Certain requirements to provide benefits for breast reconstruction after a mastectomy.
The exemption from these Federal requirements will be in effect for the 2019 plan year beginning January 1, 2019, and ending
December 31, 2019. The election may be renewed for subsequent plan years.
HIPAA also requires the Plan to provide covered employees and dependents with a “certificate of creditable coverage” when they
cease to be covered under the Plan. There is no exemption from this requirement. The certificate provides evidence that you were
covered under this Plan, because if you can establish your prior coverage, you may be entitled to certain rights to reduce or eliminate
a preexisting condition exclusion if you join another employer’s health plan, or if you wish to purchase an individual health insurance
policy.
Inquiries regarding this notice can be directed to the Milwaukee County Division of Employee Benefits, Courthouse Rm. 210, 901 N.
9th St., Milwaukee, WI 53233.
Notice to Enrollees In A Self-Funded Nonfederal Governmental Group
Health Plan For Plan Years Beginning On Or After September 23, 2010
2020 ANNUAL NOTICES
Milwaukee County 2020 Benefits | 55

56 | Milwaukee County 2020 Benefits
TOTAL REWARDS
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer
Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined
in consultation with the attending physician and the patient, for:
• All stages of reconstruction of the breast on which the mastectomy was performed.
• Surgery and reconstruction of the other breast to produce a symmetrical appearance.
• Prostheses.
• Treatment of physical complications of the mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and surgical benefits
provided under this plan. Therefore, the deductibles and coinsurance apply.
If you would like more information on WHCRA benefits, call the Employee Benefits Division at (414) 278-4198.
Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay
in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours
following a cesarean section. However, Federal law generally does not prohibit the mother’s or newborn’s attending provider, after
consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case,
plans and issuers may not, under Federal law, require that a provider obtain authorization from the plan or the issuer for prescribing a
length of stay not in excess of 48 hours (or 96 hours).
Women’s Health And Cancer Rights Act Notice
Notice Of Coverage For Newborns And Mothers
2020 ANNUAL NOTICES
2020 ANNUAL NOTICES
56 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 57
TOTAL REWARDS
Health Matters Milwaukee County is a voluntary wellness program available to all employees. The program is administered according
to federal rules permitting employer-sponsored wellness programs that seek to improve employee health or prevent disease, including
the Americans with Disabilities Act of 1990, the Genetic Information Nondiscrimination Act of 2008, and the Health Insurance Portability
and Accountability Act, as applicable, among others. If you choose to participate in the wellness program you will be asked to complete a
voluntary health risk assessment or “HRA” that asks a series of questions about your health-related activities and behaviors and whether you
have or had certain medical conditions (e.g., cancer, diabetes, or heart disease). You will also be asked to complete a biometric screening,
which will include measuring your blood pressure, weight, height, waist circumference, and a finger stick blood test to measure cholesterol
and glucose. You are not required to complete the HRA or to participate in the biometric screening.
However, employees who choose to participate in the wellness program will receive an incentive of a 30% reduction to their monthly
medical insurance premium contribution (up to a maximum reduction of $50/month) for completing the health risk assessment
questionnaire and biometric screening. Although you are not required to complete the HRA or participate in the biometric screening, only
employees who do so will receive a 30% reduction to their monthly medical insurance premium contribution (up to a maximum reduction
of $50/month).
Employees who are identified as being high risk through the biometric screening will be asked to complete a telephonic health coaching
session once a quarter during a calendar year in order to continue receiving the 30% reduction to their monthly medical insurance
premium contribution (up to a maximum reduction of $50/month). Additional incentives may be available for employees who voluntarily
participate in certain health related challenges and events that are offered throughout the program year. If you are unable to participate in
any of the health-related activities or achieve the health coaching requirement to earn an incentive, you may be entitled to a reasonable
accommodation or an alternative standard. You may request a reasonable accommodation or an alternative standard by contacting the
Benefits Division at (414) 278-4198.
The information from your HRA and the results from your biometric screening will be used to provide you with information to help you
understand your current health and potential risks, and may also be used to offer you services through the wellness program, such as
health coaching. You also are encouraged to share your results or concerns with your own doctor.
Protections from Disclosure of Medical Information We are required by law to maintain the privacy and security of your personally
identifiable health information. Although the wellness program and Milwaukee County may use aggregate information it collects
to design a program based on identified health risks in the workplace, Health Matters Milwaukee County will never disclose any of
your personal information either publicly or to the employer, except as necessary to respond to a request from you for a reasonable
accommodation needed to participate in the wellness program, or as expressly permitted by law. Medical information that personally
identifies you that is provided in connection with the wellness program will not be provided to your supervisors or managers and may
never be used to make decisions regarding your employment.
Your health information will not be sold, exchanged, transferred, or otherwise disclosed except to the extent permitted by law to carry
out specific activities related to the wellness program, and you will not be asked or required to waive the confidentiality of your health
information as a condition of participating in the wellness program or receiving an incentive. Anyone who receives your information
for purposes of providing you services as part of the wellness program will abide by the same confidentiality requirements. The only
individual(s) who will receive your personally identifiable health information is a health coach in order to provide you with services under
the wellness program.
In addition, all medical information obtained through the wellness program will be maintained separate from your personnel records,
information stored electronically will be encrypted, and no information you provide as part of the wellness program will be used in making
any employment decision. Appropriate precautions will be taken to avoid any data breach, and in the event a data breach occurs involving
information you provide in connection with the wellness program, we will notify you immediately.
You may not be discriminated against in employment because of the medical information you provide as part of participating in the
wellness program, nor may you be subjected to retaliation if you choose not to participate.
If you have questions or concerns regarding this notice, or about protections against discrimination and retaliation, please contact
Wellness Coordinator Laura Kuglitsch at (414) 278-4938.
Notice Regarding Wellness Program
2020 ANNUAL NOTICES
Milwaukee County 2020 Benefits | 57
58 | Milwaukee County 2020 Benefits
TOTAL REWARDS
We are required by law to maintain the privacy and security of your personally identifiable health information. Although Froedtert
Workforce Health and Milwaukee County may use aggregate information it collects to design a program based on identified health
risks in the workplace, Froedtert Workforce Health will never disclose any of your personal information either publicly or to Milwaukee
County, except as necessary to respond to a request from you for a reasonable accommodation needed to participate in the wellness
program, or as expressly permitted by law. Medical information that personally identifies you that is provided in connection with the
wellness program will not be provided to your supervisors or managers and may never be used to make decisions regarding your
employment.
Your health information will not be sold, exchanged, transferred, or otherwise disclosed except to the extent permitted by law to carry
out specific activities related to the wellness program, and you will not be asked or required to waive the confidentiality of your health
information as a condition of participating in the wellness program or receiving an incentive. Anyone who receives your information
for purposes of providing you services as part of the wellness program will abide by the same confidentiality requirements. The only
individual(s) who will receive your personally identifiable health information are health coaches from Froedtert Workforce Health in
order to provide you with services under the wellness program.
In addition, all medical information obtained through the wellness program will be maintained separate from your personnel records,
information stored electronically will be encrypted, and no information you provide as part of the wellness program will be used in
making any employment decision. Appropriate precautions will be taken to avoid any data breach, and in the event a data breach
occurs involving information you provide in connection with the wellness program, we will notify you immediately.
You may not be discriminated against in employment because of the medical information you provide as part of participating in the
wellness program, nor may you be subjected to retaliation if you choose not to participate.
If you have questions or concerns regarding this notice, or about protections against discrimination and retaliation, please contact the
Benefits Division at (414) 278-4198.
Protections From Disclosure Of Medical Information
2020 ANNUAL NOTICES
58 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 59
TOTAL REWARDS
55
New
and Your
PART A: General
Yes. If you have an oer of health coverage from your employer that meets certain standards, you will not be eligible for a tax cred-
it through the Marketplace and may wish to enroll in your employer's health plan. However, you may be eligible for a tax credit
that lowers your monthly premium, or a reducon in certain cost-sharing if your employer does not oer coverage to you at all or
does not oer coverage that meets certain standards. If the cost of a plan from your employer that would cover you (and not any
other members of your family) is more than 9.5% of your household income for the year, or if the coverage your employer provides
does not meet the "minimum value" standard set by the Aordable Care Act, you may be eligible for a tax credit.
As that percentage is adjusted by inflation from time to time.
An if the share of
by is no less of
Milwaukee County 2020 Benefits | 59

60 | Milwaukee County 2020 Benefits
TOTAL REWARDS
56
60 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 61
TOTAL REWARDS
57
Milwaukee County 2020 Benefits | 61

62 | Milwaukee County 2020 Benefits
TOTAL REWARDS
58
62 | Milwaukee County 2020 Benefits

Milwaukee County 2020 Benefits | 63
TOTAL REWARDS
59
Milwaukee County 2020 Benefits | 63

64 | Milwaukee County 2020 Benefits
TOTAL REWARDS
Insurance Type Provider Group Contact Number Website
Commuter Value Pass
Milwaukee County
Transit System
(414) 343-1777
www.ridemcts.com
Deferred Compensation
Empower
Retirement
Enrollment:
(414) 223-1921
Customer Service:
877-457-6459
www.milwaukeecounty457.com
Dental Insurance Delta Dental 90813
Customer Service:
800-236-3712
www.deltadentalwi.com
Employee Assistance
Program
United
Behavioral Health
Customer Service:
800-622-7276
www.liveandworkwell.com
Flexible Spending
Account
Employee Benefits
Corporation
Customer Service:
800-346-2126
www.ebcflex.com
Home & Auto Insurance Metlife 844-569-3607
www.metlife.com/insurance
Legal Plan MetLife 1-800-821-6400
www.legalplans.com/metlaw
Life Insurance Metlife 104177
Customer Service:
800-638-6420
www.metlife.com
Medical Insurance UnitedHealthcare 714852
Customer Service:
800-603-3941
www.myuhc.com
Prescription Plan OptumRx Milwcnty
Customer Service:
800-603-3941
www.myuhc.com
Supplemental
Insurance Policies
Colonial Life & Accident
Insurance Co.
Enrollment:
(414) 446-8494
Customer Service:
800-845-7330
www.coloniallife.com
Vision Insurance DeltaVision 844-848-7090
www.eyemedvisioncare.com
Wellness Program
Froedtert Workforce
Health
(414) 777-3446
https://countyconnect.
milwaukeecountywi.gov/
Employee-Wellness
2020 PROVIDERS
Department of Human Resources
Milwaukee County Courthouse • 901 N. 9th St. • Milwaukee, WI 53233 • (414) 278-4198
