
1
Equality, diversity and inclusion in
recruitment to Public Health specialty
training in the United Kingdom
A report commissioned by the UK Recruitment Executive Group of Health
Education England and the Faculty of Public Health
Fran Bury MFPH
Richard Pinder FFPH FRCP
School of Public Health
Imperial College London
Final version
Date of Publication: November 2022
2
CONTENTS
Executive Summary 3
Introduction 5
Recruitment into Public Health Specialty Training 9
Methods 14
Findings 15
Options for action 27
Recommendations for the Recruitment Executive Group 31
Conclusion 32
References 33
Appendices 35
Appendix A. Detailed results from Analysis 1: Success rates 35
Appendix B. Detailed results from Analysis 2: Staged progression pipeline 38
Appendix C. Detailed results from Analysis 3: Assessment Centre performance 43
Cite as: Bury F, Pinder RJ. Equality, diversity and inclusion in recruitment to Public Health
specialty training in the United Kingdom. 2022. Imperial College London, London, United
Kingdom.
3
Executive Summary
Public Health is a profession that seeks a more equal and more equitable world. The Public Health
specialty training scheme is the primary route to becoming a senior Public Health professional in
the United Kingdom. Over recent years recruitment into Public Health specialty training has
become increasingly competitive. The recruitment process in 2022 received more than 1000
applications for approximately 70 places.
Established in 2009, the current multi-stage recruitment process involves eligibility checking,
psychometric assessment and interview. Previous academic analysis has shown the process to
be effective in selecting candidates likely to perform well in training.
While care has been taken to design and maintain a recruitment process that attempts to be
impartial, Health Education England’s Public Health Recruitment Executive Group has been
increasingly concerned about the risk of differential attainment – a phenomenon observed in many
clinical specialties and at many different levels, where some groups appear systematically
disadvantaged in their ability to progress.
After identifying trends suggesting differential attainment from routine monitoring, the Recruitment
Executive Group invited Imperial College London to independently analyse four years of
application data to determine the extent to which differential attainment may be present and, if
present, how it may be mitigated.
The applicant pool for Public Health is highly diverse. There was no evidence to suggest that
interviewers were unfairly discriminating against minoritised groups. There was no evidence that
first language or socioeconomic status was associated with success. The main point-of-loss for
some candidate groups appears to be within the psychometric testing stage. Candidates from
ethnic minority backgrounds, those who are older, those from international medical graduate
backgrounds and backgrounds other than medicine are materially under-represented by the end
of the process. After statistical adjustment these patterns remain, leading to the conclusion that
differential attainment is present in the process.
This report presents a range of options for the Recruitment Executive Group in mitigating future
differential attainment to enable Public Health to deliver on its mission to create a fairer world.

4
Abbreviations
About the authors
Fran Bury (FB) is a Public Health registrar training in London, and a member of the Faculty of
Public Health’s Equality and Diversity Special Interest Group. Prior to entering Public Health
specialty training she worked in the private sector and local government and then ran the
operations for a children’s charity in North London.
Richard Pinder (RJP) is a consultant and clinical academic in Public Health Medicine based in
the School of Public Health at Imperial College London. RJP was the technical co-lead for
Assessment Centre from 2017 to 2021 and a member of the Recruitment Executive Group during
that time.
AC
Assessment Centre
BOTM
Background other than medicine
FPH
Faculty of Public Health
HEE
Health Education England
IMG
International Medical Graduate
RANRA
Rust Advanced Numerical Reasoning Assessment - one of the three
psychometric tests used as the Assessment Centre
REG
Recruitment Executive Group
SC
Selection Centre
SJT
Situational Judgement Test - one of the three psychometric tests used
as the Assessment Centre
WG
Watson Glaser test of critical thinking - one of the three psychometric
tests used as the Assessment Centre
5
Introduction
Background
Public Health is a medical specialty rooted in identifying and dismantling structural barriers and
the inequity they drive. In this way, Public Health as a profession has been outwardly progressive
in advocating for greater equality, diversity and inclusion (EDI) over decades. Over recent years
racism and injustice have been increasingly in the spotlight: a subject of widespread societal
concern and criticism.
Institutions (including the medical and public policy professions as a whole) are being challenged
more than ever before to demonstrate how equal, diverse and inclusive they really are. A measure
of this is the extent to which their workforce truly reflects the populations they serve.
In 2020, The BMJ published a news item reporting widespread ethnic disparities among
applicants deemed appointable for specialty training. Three-quarters of White colleagues were
deemed to be appointable in 2018 across specialties, compared to 53% of those from ethnic
minority backgrounds (Iacobucci, 2020). In this article, it was suggested Public Health recruitment
resulted in the lowest proportion of ethnic minority applicants being deemed appointable: 15%
compared to over 50% among the larger specialty training programmes.
The same report also suggested that Public Health exhibited the greatest ethnicity gap: with 36%
of White candidates deemed appointable, meaning White applicants were 2.4x more likely to be
deemed appointable than ethnic minority candidates. It has not been possible to determine the
raw data source for this analysis. And while drawing precise conclusions from these findings is
fraught with complexity, the analysis poses a valid question: is there differential attainment in
Public Health specialty recruitment?
Context
Governance and accountability
The UK Public Health Recruitment Executive Group (REG) is a committee of Health Education
England that reports to the Medical and Dental Recruitment and Selection (MDRS) Board. The
REG is responsible for overseeing the recruitment process for Public Health across the four
nations of the United Kingdom. The REG is led by two Consultant-level Co-Chairs: a regional
Head of School and a Training Programme Director. Its membership includes representatives of
Health Education East Midlands (the lead organisation for Public Health recruitment across the
four nations), the UK Faculty of Public Health, Consultant leads for the components of the
recruitment process and specialty registrar representatives.

6
Recruitment cycle and monitoring
For those outside the specialty, it is important to note that Public Health specialty training differs
from most other medical specialties. The Consultant workforce in Public Health comprises a
mixture of staff from medical backgrounds as well as backgrounds other than medicine (BOTM).
Today, this is mirrored in the eligibility for training as Public Health specialty training attracts
applicants from medical as well as BOTM backgrounds, with differing eligibility criteria applied.
As such, any recruitment process cannot assume a clinical background or indeed assess on the
basis of presumed clinical competence as is the case in most other specialities (including those
who rely on the Multi-Specialty Recruitment Assessment, MSRA).
The Public Health specialty recruitment cycle for candidates begins in November of each year,
with a three-stage recruitment process culminating the following March, when offers are made for
prospective registrars to start their training five months later in August. For the REG, the
recruitment cycle is an all-year programme with substantial planning and logistics work beginning
almost as soon as the preceding cycle has completed. For the purposes of this report, recruitment
cycles are referred to by their August intake year, meaning that the cycle that began in 2019
leading to appointments made for 2020, is referred to as the 2020 cycle.
A more detailed description of the recruitment process is included later in this report. However,
the quality assurance of the recruitment cycle has been reported every year in a late Spring-time
wash-up meeting since the current multi-stage process was introduced in 2009. Demographic
and equalities monitoring has been subject to scrutiny throughout that period. The current
recruitment design was successfully validated against postgraduate progression in terms of
annual appraisal and postgraduate examinations (Pashayan et al., 2016). However no similar
process beyond routine monitoring had been devised in relation to differential attainment. This
routine monitoring has demonstrated an association of non-White ethnicity and older age with
lower overall performance although single-year cohorts have until now precluded more robust
analyses. While a number of explanatory hypotheses have been proposed, there was insufficient
analytical capacity to test these properly. Efforts have been made over the period to prevent
differential attainment: unconscious bias training and a number of other safeguards have been
implemented following concerns that the interview panels might be unduly favouring certain
applicants.
Differential attainment
The UK General Medical Council defines differential attainment as the gap between attainment
levels of different groups of doctors, which exists in multiple contexts including recruitment,
examination, progression (General Medical Council, 2022). The GMC defines differential
attainment to be inherently unfair.
Commonly, the term discrimination, implies a process that is unfair. However, in one sense
discrimination is a technical process of differentiating one group from another and ultimately the

7
goal of all selection processes. While it is clear that discrimination relating to a protected
characteristic (within the Equality Act 2010, and associated Public Sector Equality Duty) is
absolutely unacceptable, the extent to which some elements of professional values and behaviour
are culturally underpinned can present challenges when trying to determine what outputs of a
selection process are intended (versus unintended), and acceptable (versus unacceptable).
For example, professional attitudes differ around the world in relation to punctuality. Therefore, it
is possible to debate the fairness of evaluating an applicant’s attitude towards punctuality through
a situational judgment test.
a
Likewise, in a professional environment where communication
capability is important, the extent to which English language proficiency (or lack thereof) is
intentionally or acceptably assessed can be questioned.
Differential attainment in medical training has been observed across many clinical specialties,
although research has traditionally focused on postgraduate examinations and progression
(McManus & Wakeford, 2014; Patterson et al., 2018; Tiffin & Paton, 2021). Much of the evidence
in medicine has focused on three groups: white UK medical graduates, non-White UK medical
graduates and international medical graduates (IMG) with clear trends showing poorer
progression statistics for the latter two groups when compared to the former.
Yet evidence is increasingly showing that differential attainment in respect of ethnicity occurs
early, even during undergraduate training (Gupta et al., 2021). While beliefs persist that such
disadvantage is attributable to biased examiners and selectors (Woolf, 2020), differential
attainment is observed on machine marked assessments too (Woolf et al., 2013).
Comparatively less has been reported on recruitment processes in UK medical specialty
recruitment.
Terms of reference and reporting
It was in the context described so far, that the REG commissioned Imperial College London in
late 2021 to independently:
1. Investigate the extent to which differential attainment may be present in the recruitment
process for Public Health specialty training; and
2. Make recommendations to mitigate any adverse impacts identified.
By this time, the REG had already introduced enhanced EDI monitoring for the 2021 cycle
recognising the need for better data to understand the problem. This report’s senior author made
recommendations for that data collection process in his position as a member of REG and
Technical Co-Lead for the Assessment Centre process in 2020.
a
Situational judgment tests are used widely in the selection of applicants in postgraduate medical
recruitment in the United Kingdom. Clinical assessments commonly involve providing a candidate with a
scenario after which they are invited to rank or select actions / responses (Koczwara et al., 2012).
8
This technical report and accompanying peer-reviewed publications form the outputs of this
commission.
Neither Health Education England (and its committees) nor the Faculty of Public Health had any
role in the analysis, reporting, recommendations or decision to submit findings presented in this
report or associated peer-reviewed publications. Owing to the timelines involved in peer-review,
the REG were given access to the findings ahead of public release.
This report is the work of the named authors who independently analysed the data and present
their recommendations.

9
Recruitment into Public Health Specialty Training
The Public Health Specialty Training recruitment process
Since the introduction of the current multi-stage process in 2009, Public Health recruitment has
extended from an England and Wales system, to incorporate Scotland, Northern Ireland, Defence
and Dental Public Health. As part of the preparation for the 2009 launch, detailed work was
undertaken to define the job description and person specification of the Specialty Registrar. The
intent was that the newly designed recruitment process would enable HEE to select the strongest
candidates into specialty training.
Candidates applying for specialty training in Public Health are assessed at three points to
determine whether they meet the person specification
b
and are appointable:
▪ Eligibility checking - candidates are required to demonstrate they meet the eligibility
criteria as set out in the person specification:
▪ Medical route: have completed a primary medical qualification, be eligible for full
registration with, and hold a current licence to practise from, the UK General
Medical Council (GMC), have a minimum of two years of postgraduate medical
experience (equivalent to the UK Foundation Programme) and have evidence of
having achieved foundation competencies in the last three years.
▪ BOTM route: have completed an undergraduate degree (1st or 2:1 or equivalent)
OR a higher certified degree (e.g. MSc, PhD), have at least 48 months of full time
work experience at the time of application, of which at least 24 months must be in
an area relevant to population health practice. The 24 months should be at Band
6 or above of Agenda for Change or equivalent, and a minimum of three months
at Band 6 or above should have been in the last three years.
All candidates who meet these criteria are then invited to the Assessment Centre
▪ Assessment Centre - candidates sit three psychometric tests over a period of
approximately three hours:
▪ Watson Glaser II Critical Thinking Appraisal (WGCTA II): a test of critical thinking
widely used across the world in recruitment to professional roles.
▪ Rust Advanced Numerical Reasoning Assessment (RANRA): a test of numerical
reasoning developed specifically for the UK market
▪ Situational Judgement Test (SJT): developed specifically for the Public Health
Specialty Training programme, this tests four characteristics from the person
specification (managing others and team involvement; professional integrity;
b
Person specification for 2023 recruitment round can be found at
https://specialtytraining.hee.nhs.uk/portals/1/Content/Person%20Specifications/Public%20Health/PUBLIC
%20HEALTH%20-%20ST1%202023.pdf
10
coping with pressure; organisation and planning).
In order to pass the Assessment Centre, candidates must achieve a standardised pass
score on all three tests.
For the 2022 cycle, to be invited to the Selection Centre, candidates must rank in the top 216
following Assessment Centre (or, for candidates eligible via the Disability Confident Scheme, pass
all three tests). The number of places at Selection Centre is broadly stable around 216 both prior
to and since the pandemic, but a reserve list is also sometimes called upon if candidates at or
above 216 withdraw. Rank is calculated based on an overall Assessment Centre score, with
Watson Glaser and RANRA weighted 25% each, and the SJT weighted at 50%.
▪ Selection Centre - until 2020 this was an in-person event held in Loughborough, and
assessed candidates via a written exercise, a group exercise and six mini-interviews
taking approximately three hours. Since 2021, due to the COVID-19 pandemic, the
Selection Centre-equivalent has been held online, and the components reduced to a
single multi-question interview taking place over approximately 40 minutes.
At the end of the Selection Centre process, candidates are deemed appointable if they
pass a threshold score normally considered as 60% of the marks available in the Selection
Centre.
Those deemed appointable at Selection Centre are again ranked for a final recruitment score
comprising 60% of their score coming from Selection Centre, and 13.3% from each of the
Assessment Centre tests.
Posts are then offered to candidates, reflecting their location preferences as stated in their
application, starting with the top-ranked candidate and working down the list until all posts have
been filled.
The high-level process is summarised visually with approximate numbers (Figure 1).
As the number of applicants has grown (now exceeding 1000 candidates in the 2022 cycle), the
system has increasingly acted as a funnel with scrutiny increasing as candidates progress.
Accordingly, candidates are only deemed appointable after successfully completing all three of
these recruitment stages. It is likely that this bottleneck (constraining the numerator) and a very
large number of applicants applying but removed at earlier stages of the process (contributing to
the denominator) is part of the reason for the much lower percentages of candidates deemed
appointable (from both White and minority ethnic groups) cited in The BMJ analysis.

11
Figure 1. Funnel overview of the Public Health Specialty Training recruitment process,
extract from monitoring report (2021).
Existing actions undertaken to reduce the risk of differential attainment in
the process
Since its establishment, the REG has monitored the recruitment process and attempted to identify
groups which may be under-represented through the process.
In the first years after the establishment of the national recruitment process, the REG
commissioned an academic to assess the predictive validity of the new process, assessing scores
in recruitment against measures of progress through training. This analysis showed that higher
scores in the various parts of the recruitment process were associated with higher odds of passing
professional exams in training, and making satisfactory progress through training (assessed by
Annual Review of Competence Progression (ARCP) outcomes) (Pashayan et al., 2016). Related
(and unpublished) analysis by the private company who co-designed the 2009 process suggested
that the process demonstrated lower differential attainment than the regional processes it
replaced (Work Psychology Group, 2021).
There are various ways in which the REG, in designing and running the recruitment process, has
attempted to reduce the risk of differential attainment (Table 1).

12
Table 1. Existing measures to reduce the risk of differential attainment in the recruitment
process
Stage
Measures
Application
process
Public Health training is open to candidates from a wide range of professional
backgrounds, potentially increasing the diversity of the pool of applicants.
Since 2020 and inclusion on the UK Shortage Occupation List, the
recruitment into specialty training has been open to those requiring visa
sponsorship to work in the UK.
Eligibility
checking
Eligibility checkers are blinded to candidates’ name, age and sex. However,
they can identify country of primary qualification, location of work experience
and may be able to deduce age from other information provided. All eligibility
checkers are trained to ensure consistency in who is deemed eligible. All
applications are judged by two people independently, and a process exists
for resolving disagreements when these arise.
Assessment
Centre
Tests are the same for all candidates, regardless of professional background.
When introduced, all three tests were tested against existing measures (prior
to the introduction of a single national recruitment process) and found to
result in lower levels of differential attainment. Situational Judgement Tests
are developed through a rigorous process involving subject matter experts,
and tested and piloted before being used.
Selection
Centre
Interviewers are blinded to applicant’s background. Interviewers are required
to have undertaken Equality and Diversity training and Unconscious Bias
training. As far as possible, a diverse pool of interviewers is recruited
Each part of the process is marked by two or three assessors. Prior to the
pandemic at least 10 people assessed each candidate. Since the switch to
interview format, two people assessed each candidate in 2021 and three
people in 2022.
Process
overall
The recruitment process combines scores from a range of different types of
test, covering a range of competencies, to create a balanced overall score.
In 2020, ahead of the 2021 recruitment cycle, two additional voluntary questions were
incorporated into the initial application process designed to facilitate subsequent analysis for
possible residual confounders. The questions were designed to approximate language and
socioeconomic status.
The two questions posed were:
1. What is your main language?
Sourced from UK Census 2011 (Office for National Statistics, 2009)
13
2. What is the highest level of qualifications achieved by either of your parent(s) or
guardian(s) by the time you were 18?
Sourced from Cabinet Office paper on measuring proxies of socioeconomic status (HM
Government, 2018)
Furthermore, we also reviewed all medical applicants to identify whether they were UK trained or
non-UK trained (international medical graduate, IMG).
It is important to note that some medically qualified persons apply through the BOTM route due
to them not being able to fulfil the medical eligibility criteria – whether to do with recent clinical
competence or because they are not registered or eligible for a licence to practise in the UK. This
number is likely to be small, but the exact number is unknown. These candidates are categorised
in the following analyses as BOTM applicants.
14
Methods
Data extracts were provided to the analytical team by Health Education East Midlands. These
were partially redacted to fulfil data protection requirements on data minimisation. Four datasets
were provided, including applicant-level demographic and performance data across the four years
from 2018 to 2021 inclusive. Data were stored securely in-line with local information governance
requirements, and analyses were undertaken using STATA 17.0 for Mac.
The complexity of the recruitment process and potentially multiple (dependent variable) endpoints
necessitated a hypothesis-driven approach. Accordingly, and ex ante, a pre-specified descriptive
analysis and the following four hypotheses were selected following engagement with key
stakeholders:
H1. Lower success rates among non-White candidates reflected poorer performance by
International Medical Graduates
H2. Lower success rates among non-White candidates reflected a smaller proportion of
non-White candidates having English as a first language than White candidates
H3. Lower success rates among non-White and older candidates are confounded or
mediated by professional background
H4. Older candidates may have applied multiple times in the past and been unsuccessful
- could not be tested as data on the number of attempts made by candidates is not
collected.
The recruitment cycle interviews (termed ‘Selection Centre’) completed just as the pandemic
manifested in 2020. In-person interviews were not possible in 2021, meaning that the method of
selection changed. Accordingly, comparisons between the process up to 2020 and in 2021 and
beyond are not directly comparable. The 2021 recruitment cycle also collected the enhanced
equalities data. Therefore, two analytical cohorts were designated: the first covering the three
years 2018-2020 and the second, a single year snapshot of 2021.
The extracts were cleaned, collated and compiled into two cohorts for the analytical processes.

15
Findings
Preface
This report is underpinned by the peer-reviewed scientific papers that accompany it. Full methods
statements are included in those papers.
Please note that there are a very large number of potential endpoints that can be used to
characterise progression in this process.
Cohort sizes
There were 2430 applications to specialty training in the three years 2018 to 2020 inclusive (Table
2). For the second cohort (2021, involving the enhanced equalities monitoring), there were 984
applicants (Table 3).
Table 2. Descriptive breakdown of cohort by group, 2018-2020.
Application
year 2018
Application
year 2019
Application
year 2020
Total
applications
made
n
(%)
n
(%)
n
(%)
N
Total [%]
732
[30.1]
769
[31.7]
929
[38.2]
2430
Sex [%]
- Male
- Female
- Not disclosed
238
478
16
(32.5)
(65.3)
(2.2)
232
507
30
(30.2)
(65.9)
(3.9)
296
605
28
(31.9)
(65.1)
(3.0)
766
1590
74
Age group [%]
- ≤29
- 30-34
- 35-39
- 40-44
- 45+
- Not disclosed
229
211
159
73
60
-
(31.3)
(28.8)
(21.7)
(10.0)
(8.2)
218
207
171
84
70
19
(28.3)
(26.9)
(22.2)
(10.9)
(9.1)
(2.5)
261
275
184
101
77
31
(28.1)
(28.5)
(21.2)
(10.6)
(8.5)
(2.1)
708
693
514
258
207
50
Ethnicity [%]
- White British
- White Other
- Black
- Asian
- Mixed
- Chinese
- Other
- Not disclosed
346
84
84
119
37
8
11
43
(47.3)
(11.5)
(11.5)
(16.3)
(5.1)
(1.1)
(1.5)
(5.9)
390
66
80
113
25
16
19
50
(50.7)
(8.6)
(11.7)
(14.7)
(3.3)
(2.1)
(2.5)
(6.5)
455
81
112
155
43
13
18
52
(49.0)
(8.7)
(12.1)
(16.7)
(4.6)
(1.4)
(1.9)
(5.6)
1191
231
286
387
105
37
48
145
Professional
background [%]
- Medical
- BOTM
- Not disclosed
328
404
-
(44.8)
(55.2)
332
437
(43.2)
(56.8)
378
551
(40.7)
(59.3)
1392
1038

16
Table 3. Descriptive breakdown of cohort by group, 2021.
Application year 2021
n
(%)
Total
984
Sex [%]
- Male
- Female
- Not disclosed
315
641
28
(32.0)
(65.1)
(2.8)
Age group [%]
- ≤29
- 30-34
- 35-39
- 40-44
- 45+
- Not disclosed
306
269
165
115
77
52
(31.1)
(27.3)
(16.8)
(11.7)
(7.8)
(5.3)
Ethnicity [%]
- White British
- White Other
- Black
- Asian
- Mixed
- Chinese
- Other
- Not disclosed
438
90
123
170
57
13
38
55
(44.5)
(9.1)
(12.5)
(17.3)
(5.8)
(1.3)
(3.9)
(5.6)
Professional
background [%]
- UK Medical
- IMG
- BOTM
- Not disclosed
290
155
539
-
(29.5)
(15.8)
(54.8)
Highest parental
qualification
- No degree
- Degree
- Not disclosed
315
591
78
(32.0)
(60.1)
(7.9)
Main language
- English
- Not English
- Not disclosed
672
72
240
(68.3)
(7.3)
(24.4)

17
Analysis 1: Overall success rates by demographic group (2021)
To begin the analysis, we start high-level and examine the process from end-to-end. In this
analysis we use the term success rate:
c
success rate =
[candidates offered a post]
[
total candidates applied
]
− [candidates who withdrew their application]
In this analysis, we present the data broken down by demographic and professional
characteristics (Table 4). In 2021, the overall success rate was 15%
Graphs showing success rates for each group in 2018-2021 and 2021 are reported later
(Appendix A).
Analysis 1 identified suggests differential attainment, as the following groups were less
likely to be successful in recruitment to Public Health specialty training:
- Older candidates
- Non-white candidates, especially those from Black, Asian and Chinese
backgrounds
- International medical graduates and those from a background other than medicine
- Candidates who do not speak English as a first language
c
While mathematically not technically a ‘rate’, the term success rate is used as it appropriately describes the measurement
intended.

18
Table 4. Success rates by demographic group (2021 cohort)
Demographic
characteristic
Pattern seen in
recruitment in 2021
Was there evidence of differential attainment in
2021?
Sex
64% of successful
candidates are female
No. Male and female candidates are equally likely to be
successful:
- Male: 17%
- Female: 14%
(p=0.29, no statistically significant difference)
Age
83% of successful
candidates are under 35
years old
Yes. Success rate declines with increasing age
- Under 30: 25%
- 30-34: 17%
- 35-39: 10%
- 40-44: 3%
- Over 45: 5%
Ethnicity
79% of successful
candidates are White
Yes. Success rates varies by ethnicity
- White British: 22%
- White Other: 16%
- Asian: 6%
- Black: 4%
- Chinese: 9%
- Mixed: 21%
- Other: 13%
Overall, the “Mixed” category performs similarly to “White
British”
Professional
background
60% of successful
candidates are UK
Medical graduates, 3%
are IMG and 36%
BOTM
Yes. Success rates vary by professional background
- UK Medical graduates: 36%
- IMG: 4%
- BOTM: 9%
Primary
language
96% of successful
candidates reported
English as their primary
language (NB. data
were not available for
24% of candidates)
Yes. Success rates vary by first language
- English: 17%
- Not English: 8%
Highest
educational
qualification of
either parent
(SES proxy)
68% of successful
candidates had one or
more parent with a
degree level
qualification
No. Success rates did not vary by parental education
level
- No qualifications: 15%
- Qualifications below degree level: 14%
- Degree level or above: 16%

19
Analysis 2. Staged progression “pipeline”
On the back of findings that differential attainment appears to be present, we took a stage-by-
stage approach to identify at which point(s) the differential attainment may be arising.
A pipeline visualisation is used to present the demographic proportions at each point, running
from left to right. An example of this using ethnic groups for UK medical graduates only is
presented (Figure 2). Note that the numbers in each column fall from left to right, as some
candidates fail to progress to the next stage of recruitment.
Figure 2. Recruitment “pipeline” for UK Medical Graduates, by ethnicity (2021 cohort)
This initial analysis suggests that differential attainment by ethnic group appears to be operating
even within the sub-cohort of UK medical graduates, with White British candidates forming an
increasing share of the candidates left in the recruitment process at each stage except being
deemed eligible and being offered a post. Concurrently there a notable reduction in the share of
Black candidates at the Assessment Centre, and in Asian candidates being deemed appointable.
Full pipeline diagrams can be found in Appendix B. These cover the 2021 cohort only, but similar
patterns are observed for the 2018-2020 cohort, for those characteristics for which data are
available.
Analysis 2 identified that different groups are affected at different stages of the process,
but that the greatest impact is seen at the Assessment Centre stage. The largest variation
in likelihood to progress by age, ethnicity and professional background occurs at this
stage.
20
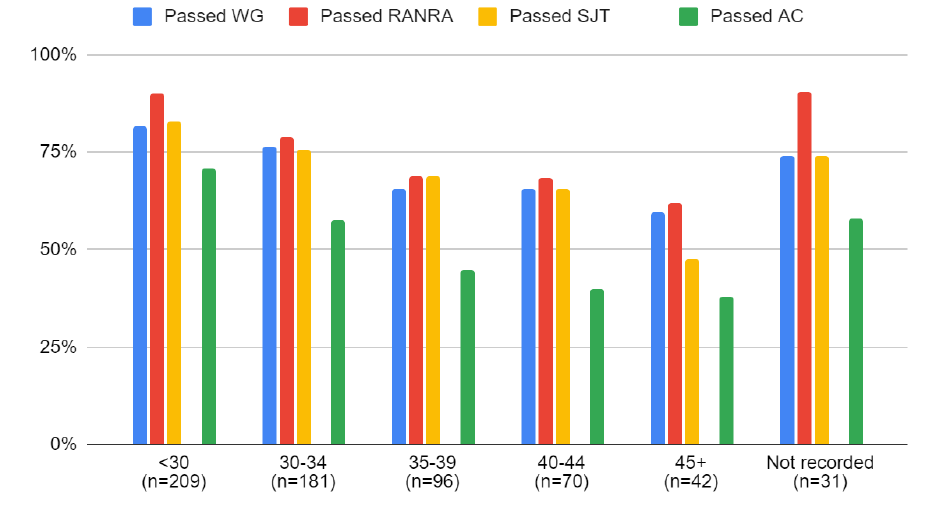
Analysis 3. Assessment Centre performance
Having identified that the most significant differential attainment by age, ethnicity and professional
background is observed in the Assessment Centre, we were interested to explore which
constituent tests, or combination of tests, might be driving the differential attainment.
As with success rates, performance on each psychometric test, and overall pass rates, were
examined by demographic group (Figure 3).
Figure 3. Assessment Centre performance by age (2021 cohort)
The full analysis can be found in Appendix C.
Analysis 3 determined that similar patterns of performance were observed across all three
psychometric tests. Groups which tend to have higher pass rates on one test also tend to
have higher pass rates on the other two. Black and Asian candidates, older candidates,
those who do not speak English as a first language and those from IMG and BOTM
backgrounds have lower overall success rates at the Assessment Centre.

21
Analysis 4. Multivariable analysis for assessment and selection
Multivariable logistic regression was undertaken for each of the cohorts against two endpoints
(dependent variables, see below). Odds ratios (OR) and adjusted odds ratios (AOR) with
accompanying 95% confidence intervals (CI) were calculated for each demographic group at two
key stages of the process:
- Passing the Assessment Centre.
Note: that this is about passing the AC, not about ranking in the top 216 candidates to
progress.
- Being deemed appointable at the Selection Centre.
Note: that this is about passing the SC, not about ranking in the top 70+ places to secure
an offer of a post.
For the purposes of presenting these data, where p<0.05 the OR is presented, while findings that
did not achieve statistical significance (alpha = 0.05) are described as “NS” or not significant.
We found few differences between the OR and AOR calculated, suggesting that each of the
demographic characteristic variables is influencing success rates independently, and there is
comparatively little confounding (at least among the variables included) taking place (Table 5).

22
Table 5. Summary results from multivariable analysis
d
Demographic
characteristic
Passing the Assessment Centre
Deemed appointable
at Selection Centre
2018-2020
2021
2018-2020
2021
Sex
NS
NS
NS
NS
Age
With increasing
age, reduced odds
of success
With increasing
age, reduced odds
of success
Candidates 45+
reduced odds of
success
NS
Ethnicity
Black OR=0.10
Asian OR=0.24
Black OR=0.17
Asian OR=0.36
Chinese OR=0.27
White Other
OR=0.56
Asian OR=0.2
Background
BOTM OR=0.38
IMG OR=0.06
BOTM OR=0.2
NS
NS
First language
N/A
NS
N/A
NS
Parental education
N/A
NS
N/A
NS
Statistical note: The OR can be interpreted as [ 1.00 – (OR) = reduction in probability of achieving the specified endpoint ].
Therefore for an OR of 0.10, it means the group had a 90% lower probability of passing AC or being deemed appointable at SC.
Analysis 4 identified statistically significantly lower probability of passing the Assessment
Centre for the following groups:
- Older candidates, with each older age band having lower likelihood of success than
the last
- Black and Asian candidates
- Chinese candidates (2021 analysis only) – note small numbers
- International medical graduates and candidates from a background other than
medicine
The analysis also identified statistically significantly lower likelihood of being deemed
appointable at Selection Centre for the following groups:
- Candidates aged over 45 (2018-2020 analysis)
- White Other candidates (2018-2020 analysis)
- Asian candidates (2021 analysis) – note small numbers
d
NS = No statistically significant differences found; N/A = this data was not collected in this period.
Reported odds ratios are unadjusted.
Reference groups were:
- Age: under 30
- Ethnicity: White British
- Background: UK Medical Graduates
- First language: English

23
Summary of findings from Public Health recruitment data
The analyses outlined above were used to test the three hypotheses (H) formulated at the start
of our research:
H1. Lower success rates among non-White candidates reflect poorer performance by
International Medical Graduates
▪ International Medical Graduates have the lowest success rate of the three
professional groups.
▪ However, within the UK Medical Graduate group, which has the highest overall
success rate, non-White candidates have lower success rates
H2. Lower success rates among non-White candidates reflect a smaller proportion of non-White
candidates having English as a first language than White candidates
▪ Candidates who speak a language other than English as their first language
have lower success rates than those who speak English as their first language
▪ However, within the group of candidates who speak English as a first language,
non-White candidates have lower success rates
H3. Lower success rates among non-White and older candidates are confounded or mediated
by professional background
▪ For example, UK Medical Graduates tend to be younger than BOTM candidates,
and tend to have higher success rates, so professional background could be
confounding the relationship between age and success.
▪ However, analysis within each professional group shows the same patterns of
lower success rates for non-White candidates and candidates aged over 35.
None of the hypotheses can either fully or collectively explain the differential attainment observed
in these analyses.
Put together, the analyses provide evidence that some demographic groups, especially
older candidates, Black and Asian candidates and candidates who are not UK medical
graduates, are less likely to be successful in recruitment to Public Health specialty
training.
This attainment gap is most marked at the Assessment Centre stage of the process, and
persists in multivariable analysis, suggesting that age, ethnicity and professional
background each are independently associated with a candidate’s likelihood of success.
24
Discussion
The analyses enable us to describe patterns of differential attainment. However, the findings
cannot explain the drivers of such patterns. To try to understand this, and what options might be
practicable and effective, we undertook a rapid literature review, with particular focus on
psychometric testing.
We focused on psychometric testing because:
▪ The most marked differential attainment in the Public Health specialty training recruitment
process is apparent the Assessment Centre, both in proportional and numerical terms.
▪ More intuitive explanations for differential attainment, such as bias by interviewers, do not
appear to explain the patterns observed.
The published literature reveals similar patterns of attainment by age and ethnicity to those
observed in Public Health specialty training recruitment. The Assessment Centre is provided by
Pearson Vue, a commercial testing and certification provider operating internationally. Pearson
Vue’s own literature on the Watson Glaser Critical Thinking Assessment reports that language,
age and especially ethnicity have been previously associated with differential group performance
on the test, but argues that following up the cohorts, there was no difference between groups
when predicting progression in-role (Pearson, 2020). Similar patterns are observed in other
cognitive ability tests (Hough et al., 2001). In associated technical documentation, it is
recommended that local implementation organisers validate attainment in their own cohorts
(Watson & Glaser, 2010).
Equivalent evaluation evidence for the RANRA test was not available, although suggestion is
made in the technical guidance that local implementors give due to consideration for candidates
with English as a second language, as the RANRA test is predicated on proficient English (Rust,
2006).
The Situational Judgment Test for Public Health is a bespoke assessment with development led
by Work Psychology Group who validate items co-developed with Public Health specialists on a
rolling basis. Annual reporting is provided back to the REG which includes analysis of group
performance. There has been a consistent pattern of differential performance by ethnicity and
professional group in those reports.
In summary, the evidence from the literature available on cognitive testing suggests that ethnic
and age differences are at best not unusual and, at worst, commonplace (Hough et al., 2001).
The causes of differential attainment in psychometric testing are unknown, although a number of
hypotheses have been proposed:
▪ Differential access to networks of people who can support preparation for the recruitment
process
▪ Differential familiarity with psychometric testing generally, and the specific tests used

25
(Hinton, 2014)
▪ Test taker perception (candidates perform better on tests which they perceive to have
higher criterion validity) (Hough et al., 2001)
▪ Test taker concern or stereotype threat (poorer performance by candidates who belong
to groups who are not expected to perform well on tests)
(Steele, 1997)
▪ Structural racism as experienced throughout the life-course (in education and more
broadly)
Of interest, tests focusing on other domains have been shown to have different patterns of
differential attainment. For example, tests of emotional intelligence, interpersonal skills and
performance on real job tasks, have be found to show less differential attainment or even favour
minoritised groups and older candidates (Hough et al., 2001).
A number of approaches have been taken in other recruitment settings to try to overcome historic
differential attainment:
▪ The Royal College of Midwives has developed their programme Turning the Tide which
offers mentoring and interview preparation for non-White midwives to support their career
progression
▪ A commercial recruitment specialising in improving workplace diversity, Rare Recruitment
has developed a process for contextualising the academic achievements of graduates
from less traditional backgrounds, enabling them to access elite graduate schemes, for
example in law firms.
▪ Rare Recruitment also offers internships and coaching to support non-White candidates
to prepare for the selection processes of specific employers, including Civil Service Fast
Stream. Such schemes produce substantial improvements in the likelihood of candidates
being successful (Rare Recruitment, 2012)
While this is the largest and most comprehensive analysis to date on these data, there are
inherent limitations to this analytical process. Even with the aggregation of multiple years’ data,
the findings are limited by comparatively small group sizes for minoritised groups. The analytical
mitigation was to aggregate ethnic groups which consequently risks masking underlying
differences between more precise ethnic groups.
The enhanced equalities monitoring questions were introduced in the 2021 recruitment cycle (and
have been retained for 2022 onwards). However, we note no positive findings for either of the two
new questions. Like the other negative findings, the possibility of a type II error cannot be
discounted (where the absence of a finding does not mean the absence of an effect).
The risks of misclassification have already been highlighted. The findings of differential attainment
for IMG are stark and consistent with patterns observed elsewhere. It is likely that there are IMGs
and possibly UK trained doctors misclassified as BOTM and future data collection should focus
on capturing this variable more accurately.
26
Finally, because the numbers reduce as the process advances, the statistical power to identify
issues at the Selection Centre stage is less than that at earlier stages of the process. While we
are confident that differential attainment appears more attributable to the Assessment Centre than
the Selection Centre, we also cannot rule out differential attainment occurring at the Selection
Centre. The implication of this is that attention should continue on ensuring an EDI-informed
approach among assessors.
27
Options for action
These analyses point to the need for action to be taken to ensure the Public Health specialty
training recruitment process is fair for all applicants, and to ensure that Public Health as a
discipline does not lose excellent candidates because of the design of the selection process.
Possible options for action should be considered in the context of the following points:
▪ Pragmatism is vital. It is not sufficient to criticise an existing process if no better process
can be selected to replace it.
▪ The recruitment process involves hundreds of applicants each year meaning that solutions
need to be scalable.
▪ That the specialty recruitment process is part of a wider system and does not exist in
isolation; while the REG has the power to determine the process end-to-end through the
recruitment, we must recognise that options may need to be considered pre-application
and across a range of organisations and institutions and outside the HEE’s sphere of
control.
There are two further complications:
▪ Continued evidential uncertainty about the root causes of the differential attainment.
▪ The absence of ready-made solutions which could be adopted by the REG.
In light of this uncertainty, a range of options are presented chronologically (Figure 4) for
consideration (Table 6). Not all may be practical or desirable, and the risks associated with
different options are not explicitly explored. However, in the context of this report’s analyses,
doing nothing is unlikely to remain an option.

28
Figure 4. Stages of the recruitment process and areas for action

29
Table 6. Options appraisal
Areas for action
Options for action include…
1. The decision to apply
1.1 Provide universal
information and advice
prior to application
▪ Advertise and operate a national webinar prior to application
deadline, or for all those who have applied, to explain the
recruitment process and answer any questions.
▪ Provide all candidates with more information about the
Assessment Centre tests, including sample questions and model
answers with rationale.
▪ Review where training posts are advertised to increase awareness
of the recruitment opportunity
1.2 Provide targeted
support to candidates
▪ Develop a package of support focused specifically on the
recruitment process available to members of groups known to be
disadvantaged by the current process. For example, Black and
Asian candidates who were deemed eligible but not appointable in
Year 1, could be offered additional support before re-applying in
Year 2.
▪ Provide general coaching and / or mentoring support available to
members of groups known to be disadvantaged by the current
process.
2. Assessment Centre
2.1 Amend “cut scores” for
Assessment Centre tests
▪ Lower the cut scores (pass marks) for Assessment Centre tests
would increase the number of candidates eligible to attend the
Selection Centre (Pearson, 2020). However, this is likely to have
a limited impact on differential attainment unless the number of
Selection Centre slots were increased, since there are already
more candidates who pass the Assessment Centre than can be
invited to the Selection Centre, so only those with the highest
ranking proceed.
e
▪ Implement different cut scores for different groups, to reflect
established differences in performance such as those identified in
Pearson’s assessment of the Watson Glaser test.
2.2 Amend, replace or
eliminate the
psychometric tests used
at Assessment Centre
▪ Identify psychometric tests that measure the same domains
(critical thinking, numerical reasoning and situational judgement)
but show lower differential attainment than those currently used,
and either piloting them alongside existing tests or replacing
existing tests
▪ Include psychometric tests that measure different domains that
have been shown to have different patterns of differential
attainment compared with those currently used e.g. tests of social
and emotional intelligence
▪ Identify tests used by other organisations e.g. Civil Service Fast
Stream which has moved away from using generic psychometric
e
Sensitivity analysis was undertaken to assess the potential impact of changes to both cut scores and the weighting of the different
psychometric tests, and none of the changes trialled were found to significantly reduce differential attainment by ethnicity, although
there were some improvements for older candidates and those from a background other than medicine. This appeared to be a by-
product of the mismatch between candidates passing AC and the limited 216 places at SC.

30
tests and is likely to be monitoring the effect of this change on
differential attainment. It may be that these organisations are
willing to share the tests with HEE for use for Public Health
recruitment.
2.3 Replace the
Assessment Centre with
another shortlisting
approach
▪ Identify alternative ways to reduce the number of candidates to
the 216 who can be accommodated at the Selection Centre. It
should be noted that other approaches, such as scoring CVs,
would be fundamentally different from the existing approach,
which aims to measure only potential to benefit from training, and
not prior experience in Public Health.
3. Selection Centre
3.1 Increase the number
of candidates invited to
Selection Centre
▪ Differential attainment is lower at the Selection Centre than the
Assessment Centre, suggesting that allowing more candidates to
reach the Selection Centre stage could reduce differential
attainment. However, there would be cost and logistical
implications for any increase in Selection Centre places, and at
present Assessment Centre scores are still used in the final
ranking of candidates, so could continue to disadvantage some
groups of candidates.
4. Research, analysis and evaluation
4.1 Continue to collect
and analyse additional
demographic information
from all candidates
▪ Continue to collect information on parental education and main
language, and ensure data on disability (which is already
collected) is available for future analysis of differential attainment
▪ Improve monitoring to capture those with medical qualifications
applying through the Background Other Than Medicine route, to
determine whether these candidates have a distinct profile
alongside the other professional background groups, and country
of Primary Medical Qualification for any candidates with medical
degrees.
4.2 Conduct further
research to understand
the drivers of differential
attainment
▪ Seek input from subject matter experts to identify opportunities to
reduce differential attainment in the recruitment process. This
might include other recruiters e.g. Civil Service Fast Stream, or
experts within recruitment consultancies
4.3 Analyse the results of
the “Leaky pipeline”
survey carried out in 2021
▪ The “Leaky pipeline” survey of current Registrars was undertaken
by the Faculty of Public Health’s Equality and Diversity Special
Interest Group in 2021 but has not yet been analysed. It focused
on experiences of applying for Specialty Training and may include
insights which could be used to inform the development of the
recruitment process to reduce differential attainment
4.4 Monitor and evaluate
the impact of any changes
to the recruitment process
▪ Consider piloting new approaches before adopting them
permanently
▪ Ensure resources are available to monitor the impact of any
changes to the recruitment process
31
Recommendations for the Recruitment Executive Group
This report has identified that specific groups appear to be disadvantaged by the current
recruitment process. The reasons for this differential attainment are complex and not fully
understood. Any changes implemented need to recognise this uncertainty. Any such changes
also need to recognise that the current system has many features designed to reduce the risk of
differential attainment, and has been demonstrated to be effective at predicting success in key
milestones during training.
We recommend action should be taken in three key areas, in parallel:
Recommendation 1
Undertake a comprehensive review of the job analysis, person specification and
selection process
We recommend that an external organisation with expertise in recruitment processes and
equality and diversity considerations should be commissioned to review each of the key
components of the recruitment process. This should involve refreshing the job analysis (last
reviewed in 2009), updating the person specification accordingly, and then reviewing the
selection process.
We do not expect that updating the job analysis alone will have an impact on differential
attainment. However, this is a necessary foundation upon which any new or modified
selection process should be built. This work is vital in being able to determine what questions
may deemed acceptable in the Situational Judgment Test component in particular.
Given the findings of the review, particular care should be given to designing a process which
reduces the likelihood of differential attainment by ethnicity or age.
Recommendation 2
Initiate shorter-term actions to mitigate the risks associated with the current process
While the more comprehensive review work is being undertaken, there are a number of
shorter-term actions that can be pursued to mitigate the risks associated with the current
process. These should include the following options (outlined in more detail in Table 5):
▪ Provide universal information and advice around the point of application: whether prior
to applications closing, following the point of application, or again at various points
within the process.
▪ Explore opportunities to provide targeted support to candidates from disadvantaged
groups. This may require piloting and evaluating how such candidates can be
32
identified and subsequently supported. It may be that the Faculty of Public Health is
best placed to co-ordinate this.
Recommendation 3
Continue monitoring, evaluation and research to better understand, support and refine
the process
Any options pursued by the REG should be accompanied by continuing monitoring and evaluation
to assess their impact on differential attainment, as well as identifying any unintended
consequences. This evaluation should be built in from the start, and should include the following
options:
▪ Continue to collect and analyse additional demographic information from all candidates
▪ Conduct further research to understand the drivers of differential attainment
▪ Analyse the results of the “Leaky pipeline” survey carried out in 2021
▪ Monitor and evaluate the impact of any changes to the recruitment process
Conclusion
Our findings provide strong evidence that differential attainment is present in the current Public
Health specialty training recruitment process. While we acknowledge the strengths of the system
in providing a scalable, multi-point assessment of candidate potential which correlates well with
future performance, we must recognise its deficiencies.
The existing process appears to select strong candidates. Yet at the same time, it appears to
disadvantage candidates from several groups: those from minority backgrounds, those who are
older, and those from international medical graduate backgrounds and backgrounds other than
medicine.
Future improvements must take care to avoid losing the positives in attempts to mitigate the
negatives. However, action is needed to create a more level playing field and ensure that the
Public Health specialty can deliver on its commitment to a fairer and more equal future.
33
References
General Medical Council. (2022). What is differential attainment? https://www.gmc-
uk.org/education/standards-guidance-and-curricula/projects/differential-attainment/what-is-
differential-attainment
Gupta, A., Varma, S., Gulati, R., Rishi, N., Khan, N., Shankar, R., & Dave, S. (2021). Differential
attainment in undergraduate medical education: a systematic review. BJPsych Open,
7(Suppl 1), S27. https://doi.org/10.1192/BJO.2021.128
Hinton, D. P. (2014). Uncovering the root causes of ethnic differences in ability testing:
Differential test functioning, test familiarity and trait optimism as explanations of ethnic
group differences.
HM Government. (2018). Annex A - Evaluation of measures of socio-economic background.
Hough, L. M., Oswald, F. L., & Ployhart, R. E. (2001). Determinants, Detection and Amelioration
of Adverse Impact in Personnel Selection Procedures: Issues, Evidence and Lessons
Learned. International Journal of Selection and Assessment, 9(1–2), 152–194.
https://doi.org/10.1111/1468-2389.00171
Iacobucci, G. (2020). Specialty training: ethnic minority doctors’ reduced chance of being
appointed is “unacceptable.” BMJ, 368, m479. https://doi.org/10.1136/BMJ.M479
Koczwara, A., Patterson, F., Zibarras, L., Kerrin, M., Irish, B., & Wilkinson, M. (2012). Evaluating
cognitive ability, knowledge tests and situational judgement tests for postgraduate
selection. Medical Education, 46(4), 399–408. https://doi.org/10.1111/J.1365-
2923.2011.04195.X
McManus, I. C., & Wakeford, R. (2014). PLAB and UK graduates’ performance on MRCP(UK)
and MRCGP examinations: Data linkage study. BMJ (Online), 348.
https://doi.org/10.1136/bmj.g2621
Office for National Statistics (UK). (2009). Finalising the 2011 questionnaire - Office for National
Statistics.
https://www.ons.gov.uk/census/2011census/howourcensusworks/howweplannedthe2011ce
nsus/questionnairedevelopment/finalisingthe2011questionnaire
Pashayan, N., Gray, S., Duff, C., Parkes, J., Williams, D., Patterson, F., Koczwara, A., Fisher,
G., & Mason, B. W. (2016). Evaluation of recruitment and selection for specialty training in
public health: interim results of a prospective cohort study to measure the predictive validity
of the selection process. Journal of Public Health, 38(2), e194–e200.
https://doi.org/10.1093/PUBMED/FDV102
Patterson, F., Tiffin, P. A., Lopes, S., & Zibarras, L. (2018). Unpacking the dark variance of
differential attainment on examinations in overseas graduates. Medical Education, 52(7),
736–746. https://doi.org/10.1111/MEDU.13605
Pearson. (2020). Watson Glaser Efficacy Report. https://us.talentlens.com/resources/watson-
glaser-efficacy-report.html
Rare Recruitment. (2012). Diversity Graduate Recruitment.
https://www.rarerecruitment.co.uk/news/civil-service-programme-bags-best-diversity-award
Rust, J. (2006). Advanced Numerical Reasoning Appraisal TM (ANRA) Manual.
34
Steele, C. M. (1997). A threat in the air. How stereotypes shape intellectual identity and
performance. The American Psychologist, 52(6), 613–629. https://doi.org/10.1037//0003-
066X.52.6.613
Tiffin, P. A., & Paton, L. W. (2021). Differential attainment in the MRCPsych according to
ethnicity and place of qualification between 2013 and 2018: a UK cohort study.
Postgraduate Medical Journal, 97(1154), 764–776.
https://doi.org/10.1136/POSTGRADMEDJ-2020-137913
Watson, G., & Glaser, E. M. (2010). Watson-Glaser TM II Critical Thinking Appraisal Technical
Manual and User’s Guide. www.TalentLens.com
Woolf, K. (2020). Differential attainment in medical education and training. BMJ (Clinical
Research Ed.), 368. https://doi.org/10.1136/BMJ.M339
Woolf, K., Mcmanus, I. C., Potts, H. W. W., & Dacre, J. (2013). The mediators of minority ethnic
underperformance in final medical school examinations. The British Journal of Educational
Psychology, 83(Pt 1), 135–159. https://doi.org/10.1111/J.2044-8279.2011.02060.X
Work Psychology Group. (2021). Personal communication.

35
Appendices
Appendix A. Detailed results from Analysis 1: Success rates
Success rates were calculated as follows:
success rate =
[candidates offered a post]
[
total candidates applied
]
− [candidates who withdrew their application]
In 2021, 984 candidates applied, 775 did not withdraw and 118 were offered posts, giving an
overall success rate of 15%.
Success rates by age
Success rates by sex

36
Success rates by professional background
Success rates by ethnicity
All four cohorts were analysed together by reported ethnicity, rather than the condensed
categories used elsewhere in this report. Between 2018 and 2021, no candidates from
Bangladeshi (n=21), Mixed White and Black African (n=32) or Any Other Black (n=18)
backgrounds were successful in public health specialty training recruitment:

37
Success rates by parental education (proxy for socio-economic status) (2021 only)
Success rates by first language (2021 only)

38
Appendix B. Detailed results from Analysis 2: Staged progression pipeline
Pipeline diagram by age
Pipeline diagram by sex

39
Pipeline diagram by professional background
Pipeline diagram by ethnicity

40
Pipeline diagrams by ethnicity and professional background
NB the diagram for International Medical Graduates is not presented here as the number of
successful candidates is too small to be able to draw meaningful conclusions, and the small
numbers mean candidates would be potentially identifiable.

41
Pipeline diagram by parental education
Pipeline diagram by first language

42
Pipeline diagram by ethnicity and first language

43
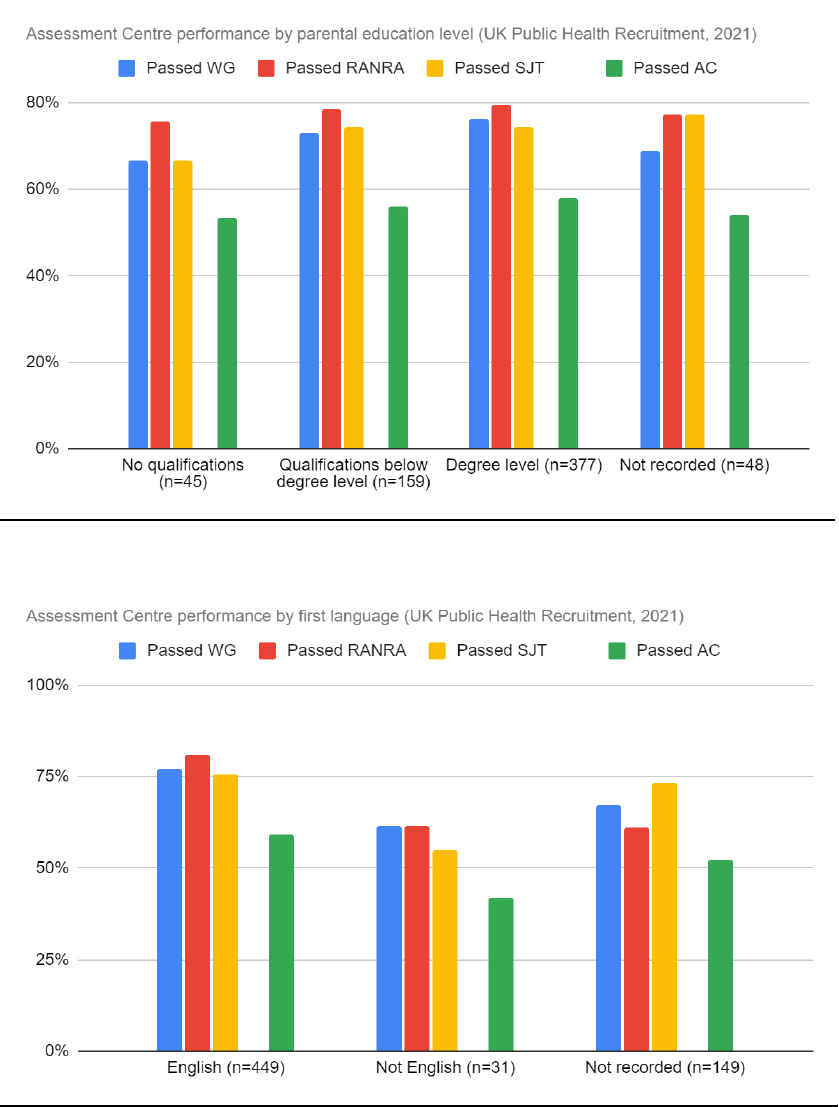
Appendix C. Detailed results from Analysis 3: Assessment Centre
performance
Assessment Centre performance by age
Assessment Centre performance by sex

44
Assessment Centre performance by professional background
Assessment Centre performance by ethnicity
45
Assessment Centre performance by parental education
Assessment Centre performance by first language
