It is a mandatory requirement that all workers and volunteers progressing with or seeking to be engaged with
the Sunshine Coast Hospital and Health Service (SCHHS) provide documentary evidence to verify that they
are either vaccinated against, or that they are not susceptible to, any of the Vaccine Preventable Diseases
(VPDs) as specified in Form B – Candidate evidence for VPD (Form B) prior to an offer of engagement.
All evidence of compliance of workers must be documented on Form B by an authorised clinician i.e., a
registered medical practitioner, authorised registered nurse (minimum NRG5 or higher) or occupational health
provider. Candidate, including medical practitioners or NRG5+, may not sign-off their own Form B application.
The candidate should avail any additional immunisation evidence (serology, immunisation statements,
childhood vaccination records, etc.) to the authorised clinician for verification and documentation on Form B.
The SCHHS Infection Management Service (IMS) is unable to accept or consider additional evidence supplied
by the candidate. Volunteers should seek advice from relevant Volunteer Co-Ordinator for instructions or
completion of form specific for volunteers.
Candidate Instructions
□
Complete tuberculosis (TB) Self-assessment Form B pages 2 to 4 prior to your appointment with the authorised clinician.
□
Take any additional immunisation evidence (serology, immunisation statements, Australian Immunisation Register
(AIR) certificates, etc.) you may have to your medical appointment for verification and sign-off on Form B by the
medical practitioner. NOTE: Candidates born from 1996 may be able to obtain sufficient evidence to provide to the
registered medical practitioner from the Australian Immunisation Register (AIR) contact 1800 653 809 or via
https://my.gov.au
and proceed to Medicare online account.
□
Sign Form B page 4 to acknowledge you have read the Privacy Notice, Consent and Certification and tick the checkbox
to certify the information provided in Form B is true and correct.
□
Authorised clinician to complete following the instructions below.
□
Return your completed signed Form B to your appointed recruitment delegate or line manager for on forwarding to
Recruitment. Do not email to IMS directly.
□
IMS does not retain documented evidence of immunity. The candidate should retain all evidence of immunity.
Authorised Clinicians Instructions
The authorised clinician (i.e., registered medical practitioner or authorised registered nurse (NRG5 or above) or
occupational health provider) is to review all pages Form B. Please complete:
□
TB screening – following review of the candidate’s TB self-assessment (Form B, pages 2 to 4), complete TB screening
on page 5 (select an appropriate item outcome checkbox to identify assessment outcome).
□
Document VPD evidence for each mandatory VPD requirement as provided for on Form B pages 6 to 8 following review
of clinical evidence on file, candidate supplied evidence, serology reports and/ or vaccine administration, (vaccine
intervals and/ or serology must be completed in accordance with the Australian Immunisation Handbook).
□
Reference Form B vaccine brands, footnotes, and further information as identified on Form B, as required.
□
Complete authorised clinician endorsement table including signature and date completed.
□
Sign and date beside all additions and amendments for mandated completion of vaccination courses to Form B
(including full name, position, provider/ registration number, clinic name & signature).
Candidate Demographics
Candidate surname: Job Reference No.
First name: Current QH payroll ID no:
Postal address:
Date of birth: Gender: Phone no.
Email:
Form B
Document ID: 000029-a2
Version: 12.0
Candidate evidence for Vaccine Preventable Disease (VPD)
Date Approved: 25/01/2023 Review Date: 25/01/2026

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 2 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
1. Cough for more than 2 weeks (not related to an existing diagnosis or condition) Yes No
2. Unexplained fever for more than 1 week Yes No
3. Recent unexplained weight loss Yes No
4. Coughing up blood Yes No
5. Excessive sweating during the night for more than 1 week Yes No
1. Were you born, and/ or have you spent three (3) months or more in total within the past five (5) years
visiting or living in country/ ies with a TB burden greater than 40 cases per 100 000 population (see
link 1b below)?
Yes
No
1a If yes, list the country/ ies:
if yes Q1,
(List countries)
1b Check the TB country incidence list
(https://www.health.nsw.gov.au/Infectious/tuberculosis/Pages/high-incidence-countries.aspx
) for
each country you have listed in questions 1a and complete the following questions:
if yes Q1
(Check high risk countries)
2. Have you been in direct contact with a person with active TB disease, without using appropriate
infection control precautions, within the past 2 years and you were not assessed for exposure to TB by
hospital or public health authorities? (Contact may be work or non-work related).
Yes
No
3. Have you previously worked (> 3 months) in any of the following settings: respiratory units; infectious
disease units or other medical units caring for infectious TB patients; clinical procedure units
conducting bronchoscopy and/or sputum induction; TB laboratories; mortuaries?
Yes
No
4. Have you ever been diagnosed with active TB (i.e., not latent TB)? Yes No
4a If yes, in what year did you complete your treatment?
If yes, Q4
(Year of treatment)
5. Do you have any underlying health issues or take any medications that cause immunosuppression? Yes No
Tuberculosis Candidate Self-Assessment (Parts A – C)
All candidates seeking to be engaged for or on behalf of the SCHHS must be assessed for their risk of Tuberculosis (TB) prior
to an offer of engagement
.
Part A – Signs of Active TB - Do you currently have any of the following symptoms?
Candidate to select Yes or No to items 1-5 below:
If you have answered YES to any questions from Part A:
➢
Make an urgent appointment with your doctor for assessment of your symptom/s. Further referral to a TB
Control Unit may be recommended by your doctor.
➢
You will require a clearance for signs of active TB from the assessing clinician (doctor or TB Control Unit) to be
provided to your recruitment coordinator / Line manager before you can be appointed to a position within the SCHHS.
Part B –TB Exposure Risk History
Candidate to select Yes or No to items 1-5 below. If required, please provide additional information where indicated:

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 3 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
In the time since encountering the risk factors in Part B, have you undergone any assessments or screening as below. If you
have previously had a test for latent TB, to avoid unnecessary repetition of testing please take (if available) any supporting
documents and additional information as indicated below to your doctor or TB Control Unit.
1. Previous employment or immigration screening for TB
No
Yes – show evidence to authorised clinician
2. Previous pathology result (QuantiFERON test or T-spot test)
No
Yes – show evidence to authorised clinician
3. Previous printed result of a tuberculin skin test result (also called
Mantoux test)
No
Yes – show evidence to authorised clinician
4. Have you ever received a bacille Calmette-Guérin (BCG) vaccine?
(This leaves a raised scar, usually on your arm near the shoulder)
No
Yes – at what age (approx.)?
If you have answered YES to any of questions 1 – 3 in Part B (above), you require a test for latent TB infection:
➢
an Interferon Gamma Release Assay (IGRA) blood test can be ordered by your doctor –
pathology fees may apply
(a positive or indeterminate IGRA result requires further consultati
on at a TB Control Unit or with your doctor. Your
doctor may refer you to a TB specialist (record results in part C).
OR
➢
a Tuberculin Skin Test (TST/ Mantoux test) can be performed by referral to a TB Control Unit – at no cost, but requires
a follow-up appointment 2 or 3 days later (record results in part C).
If testing for latent TB infection is required (and you have answered NO to all questions in Part A), you will still be able to
commence employment. However, you must undertake further assessment with a doctor and/ or at a TB Control Unit. Once
you g
et your results these should be provided to your line manager.
If you have answered
YES to any of questions 4 – 5 in Part B (above)
, you require further assessment. Contact your TB
Control Unit for advice.
NOTE there is no out
-of-pocket expense for treatment of TB in public health facilities in Queensland
Contact Tuberculosis Service Metro South Clinical Tuberculosis Service. Telephone: 07 3176 4141
Part C – Previous TB Risk Assessment Procedures & BCG History
Candidate to select Yes or No to items 1-4 below & sign:

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 4 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
Candidate Endorsement:
Please read the following notices, tick the certification checkbox and sign as indicated below:
Privacy Notice
Personal information collected by Queensland Health is handled in accordance with the Information Privacy Act 2009.
Queensland Health is collecting personal information in accordance with the Information Privacy Act 2009 in order to meet its
obligations to provide a safe workplace. All personal information will be securely stored and only accessible by authorised
Queensland Health staff.
Your personal information will not be disclosed to any other third parties without consent, unless required by law. If you choose
not to provide your personal information, you will not meet the condition of employment. For information about how Queensland
Health protects your personal information, or to learn about your right to access your own personal information, please see our
website at www.health.qld.gov.au
Consent
I consent to the recruitment panel/ human resources department giving personal information in this form to other areas within
the Queensland public sector health system (including the Department of Health and Hospital and Health Services) for workforce
planning and for outbreak management planning and response. This may include line managers and infection management
services.
I consent to my prospective employer giving personal information in this form to other areas within the Queensland public sector
health system (including the Department of Health and Hospital and Health Services) for workforce and infection management
planning and response. This may include line managers, infection control units and TB control units.
Certification
I certify that I have read and understand the Tuberculosis control protocol | Health service directive protocol | Queensland
Health risk assessment on the Queensland Health Tuberculosis website, in preparation for my employment I agree to comply
with the guidelines and all procedures in place at the Queensland Hospital and Health Service facility at which I am employed in
respect of Queensland Health vaccination and infection control of health care workers.
I certify I have read and understand the above Privacy Notice, Consent and Certification and further
confirm the information documented within Form B is true and correct.
Candidate Surname:
First Name:
Candidate Signature:
Date:
Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 5 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
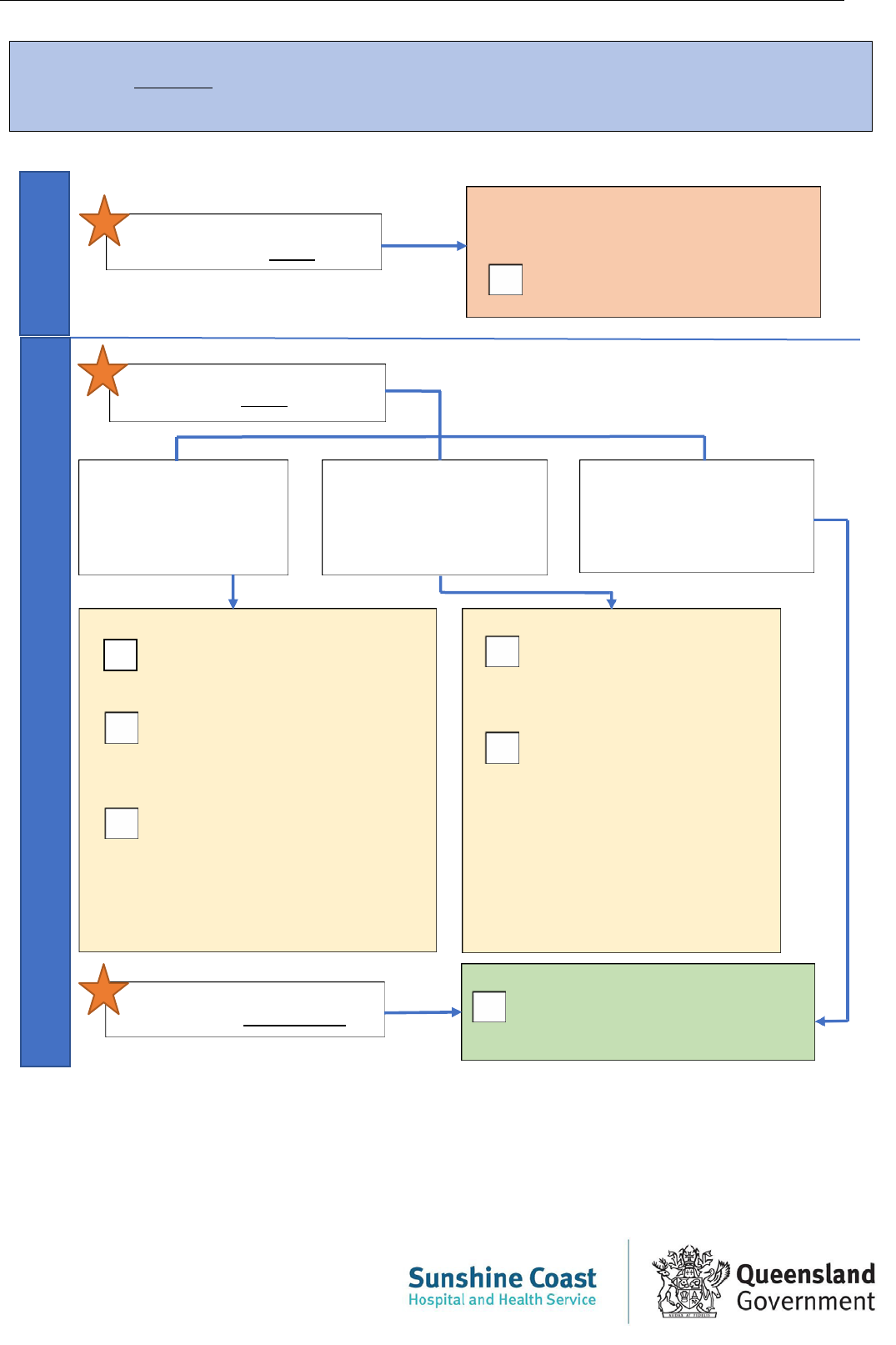
Candidate answered YES to
any/all questions in Part A
Candidate answers YES to any/
all questions in Part B
Tick appropriate action:
Clearance for active TB is required before
appointment to position – see Part A
Clearance letter from healthcare
provider for active TB is attached
Candidate answered yes
to any question in part B
(question 1-3) and no
recent assessment since
risk factor for latent TB.
Candidate answered yes
to any question in part B
(question 4-5) and no
recent assessment since
risk factor for latent TB.
Assessed by health provider
as not having TB (i.e., part
C: Mantoux, pathology done
after any risk factors listed in
part B)
Tick appropriate action:
Interferon Gamma Release Assay
(IGRA) test ordered & assessed by
healthcare provider; OR
Referred to TB Control Unit for
Tuberculin Skin Test (TST/
Mantoux test) - candidate can call
nearest unit to book; OR
Referred to medical officer
experienced in the management of
TB at site other than TB control
unit. Specify option advised
(name, location where relevant)
:
……………………………………...
Candidate answered NO to ALL
the questions in Parts A and B
Tick appropriate action:
Referred to TB Control Unit for
further advise (candidate can
call number nearest unit to
book); OR
Referred to medical officer
experienced in the
management of TB at site
other than TB Control Unit.
Specify option advised
(name,
location where relevant)
:
……………………………..……
Tick appropriate action:
Authorised Clinician Tuberculosis (TB) Screening - to be completed by the registered medical
practitioner or authorised registered nurse (NRG5 or above) or occupational health provider, following review of
candidate’s self-assessment, Form B pages 1-3. You are required to tick a relevant checkbox below:
Part
A
Part
B
No further assessment required.
Proceed to bottom of page
signature section.

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 6 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
Vaccine preventable disease evidence - to be completed by an authorised clinician (i.e., registered
medical practitioner, registered nurse (NRG5 or above) or occupational health provider).
Measles, Mumps, Rubella (MMR) People can receive MMR vaccine at the same time as other live attenuated parenteral
vaccines or other inactivated vaccines. If a person does not receive MMR vaccine at the same time as other live attenuated
parenteral vaccines, they must wait at least four weeks between live vaccinations.
Select the most appropriate option below, based on available evidence/ vaccination administration:
Candidate’s
birthdate is
before 1966
Candidate has evidence of blood
test (serology) results showing
immunity (positive IgG) for each
of measles, mumps, and rubella
1
Negative, low positive or
equivocal results will not be
accepted as true positives; 2
vaccinations are required in this
instance
Date of positive serology:
Measles IgG:
/ /
Mumps IgG:
/ /
Rubella IgG:
/ /
Candidate has had two
documented doses of
MMR vaccine at least
four weeks apart
2
Date dose 1 administered:
/ /
Date dose 2 administered:
/ /
Candidate has none of
these - commence
vaccination for MMR
2
in
accordance with
Australian
Immunisation Handbook
Candidate must not be
overdue for dose 2 prior
to commencement
Date dose 1 administered:
/ /
Varicella (Chicken Pox) People can receive varicella vaccine at the same time as other live attenuated parenteral
vaccines or other inactivated vaccines. If a person does not receive varicella vaccine at the same time as other
live attenuated parenteral vaccines, wait at least four weeks between live vaccinations.
Select the most appropriate option below, based on available evidence/ vaccination administration:
Candidate has evidence
of blood test (serology)
results showing positive
immunity (positive IgG)
for varicella
1
Negative, low positive or
equivocal results will not
be accepted as true
positives; 2 vaccinations
are required in this
instance
Date of positive serology:
/ /
Candidate is over the
age of 50 and has
documented Zoster
(shingles) vaccine:
• One dose of the
Zostavax, or
• Two doses of Shingrix
Date dose 1 administered:
/ /
Date dose 2 administered:
/ /
Candidate has two
documented doses of
Varicella vaccine, at
least four weeks apart
3
Date dose 1 administered:
/ /
Date dose 2 administered:
/ /
Candidate has none of
these - commence
vaccination for Varicella
3
in accordance with
Australian Immunisation
Handbook
Candidate must not be
overdue for dose 2 prior
to commencement
Date dose 1 administered:
/ /
Pertussis (Whooping Cough)
Candidate has had a pertussis (dTpa) containing vaccination within the past 10 years: (must not be overdue prior
to commencement
Date of dose administered: / / (n.b. ADT does not contain pertussis)

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 7 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
Hepatitis B - Not required for volunteers or administration (excluding diagnostics/ pathology collection centers/high risk
areas only).
Select the most appropriate option below, based on available evidence/ vaccination administration:
Candidate has evidence of
blood test (serology)
results showing immunity
to Hepatitis B (hepatitis B
surface anti-body titre or
anti-HBs of greater than
or equal to 10 IU/mL
4
Titre level:
IU/mL
Date of serology
4
:
/ /
Candidate has documented
doses of hepatitis B
vaccine
5
:
• Three dose schedule
5
, or
• Two doses schedule
5
if
received adult hepatitis B
vaccines between ages of
11-15 years)
Date dose 1
administered:
/ /
Date dose 2
administered:
/ /
Date dose 3
administered:
/ /
Candidate has
commenced vaccination of
hepatitis B
5
Candidate must have
completed a minimum of 2
doses prior to
commencement and must
not be overdue for the 3rd
dose prior to
commencement.
Third dose must be
administered within 6 months
of commencement.
Date dose 1
administered:
/ /
Date dose 2
administered:
/ /
Candidate is not
susceptible to
hepatitis B as has a
history of past
hepatitis B infection
6
COVID-19 All Queensland Health employees who work in or enter locations where care is provided to patients or clients, are
required to be vaccinated against COVID-19. This requirement applies to employees in both clinical and non-clinical roles
where they work in, or are required to enter, an area that a COVID-19 person (suspected or positive) may enter.
Candidate has received two doses of approved and recognized COVID-19 vaccinations
8
Date dose 1 administered:
/ /
Date dose 2 administered:
/ /
Influenza (Mandatory only for persons that work as residential aged care facilities)
Candidate is up to date with current year’s annual influenza vaccination
Date of dose administered: / /
Hepatitis A (for plumbers only)
Select the most appropriate option below, based on available evidence/ vaccination administration:
Candidate has blood test
(serology) results showing
positive Hepatitis A
surface antibodies
Date of serology:
/ /
Candidate has a
history of Hepatitis A
infection
OR
Candidate has a blood
test (serology) result
showing positive
Hepatitis A surface
antigen
Date of serology:
/ /
Candidate has two
documented doses of
Hepatitis A vaccine at
least six months apart
Date dose 1 administered:
/ /
Date dose 2 administered:
/ /
Candidate has none of
these.
Commenced (but not
completed) vaccination
for hepatitis A
Must not be overdue for
dose 2 prior to
commencement
Date dose 1 administered:
/ /_

Form B - Candidate evidence for VPD
Document No.: 000029-a2.012
Approval Date.: 25/01/2023
Page: 8 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
Endorsement & Compliance Review
Authorised Clinician Endorsement:
Registered medical practitioner/
registered nurse/occupational health
provider name & title:
Practice/ employer details including
provider/ AHPRA registration number:
Authorised clinician (Medical
practitioner e.g. GP, NRG5+,
occupational health provider)
signature:
Date:
Volunteer ONLY section (if not completed by above Authorised Clinician)
I certify that the information I have provided is true and correct.
First Name:
Surname:
Date:
Signature:
Compliance Review (SCHHS)
Reviewed by SCHHS panel chair/ delegate:
VPD compliant
VPD non-compliant
VPD exemption under application
Workforce (Recruitment) contacted and VPD exemption requested for consideration of temporary
exemption. Candidate cannot be engaged until reviewed.
Full Name
(print):
Designation
(print):
Signature:
Date:

Form B - Candidate evidence for VPD
Document ID: 000029-a2 Version: 9.0
Document No.: 000029-a2.10
Approval date: 25/01/2023
Page: 9 of 9
Printed copies are uncontrolled and will expire within 24 hours of printing
Brand names of vaccines -below list not
extensive, refer to Australian Immunisation Handbook
7
Measles, Mumps, Rubella
M-M-R-II
Priorix
Priorix-tetra
ProQuad
Pertussis
Adacel/Adacel Polio
Boostrix/Boostrix IPV
Varicella
Varilrix
Varivax
Priorix-tetra
ProQuad
Shingrix
Zostavax
Covid-19 (Refer to
Approved and
recognized COVID-19 vaccinations)
Pfizer – Comirnaty
AstraZeneca – Vaxzevria & Covishield
Moderna - Spikevax
Janssen – COVID-19 Vaccine Janssen
Hepatitis B
H-B-Vax II (adult or paediatric formulation)
Engerix-B (adult or paediatric formulation)
Infanrix hexa
Twinrix/Twinrix Junior
ComVax
Hepatitis A
Avaxim
Havrix/ Havrix Junior
Vaqta
Twinrix/Twinrix Junior
Vivaxim
Footnotes and further information
1.
Positive IgG (Immunoglobulin G) indicates evidence of
serological immunity, which may result from either
natural infection or immunisation.
2.
Pre-offer of employment requires minimum of one
dose of measles, mumps, rubella (MMR) vaccine
course. The prospective worker will be required to
commit to completing the full course. Second dose to
be administered within one month of first dose.
Vaccines given under 12 months of age are not
considered a valid dose
3.
Australian Immunisation Handbook recommends for
occupational groups as healthcare workers to
receive 2 doses of varicella vaccine if they are not
immune. Pre-offer of employment requires minimum
of one dose of varicella (chicken pox) vaccine. The
prospective worker will be required to commit to
completing the full course. Second dose to be
administered within one month of first dose.
4. Anti-HBs (hepatitis B surface antibody) greater than or
equal 10 International units/mL indicates immunity. If
the result is less than 10 International units/mL (<10
IU/mL), this indicates lack of immunity.
5.
Primary Hepatitis B vaccine course is recommended:
- 1
st
dose: day 0 (day of vaccination)
- 2
nd
dose: 1 month after 1
st
dose
- 3
rd
dose: 6 months after 1
st
dose
With minimal intervals between doses:
- 1
st
and 2
nd
dose is 1 month
- 2
nd
and 3
rd
dose is 2 months
- 1
st
and 3
rd
dose is 4 months
For adolescents between the ages of 11-15, adult
hepatitis B vaccine may be given as a two-dose
course, with the two doses 6 months apart.
Accelerated schedules are not accepted.
Pre-offer of employment requires a minimum of two
doses of Hepatitis B at least one month apart. The
prospective worker will be required to commit to
completing the full course. Third dose to be
administered within Hepatitis B vaccine course
recommendations
5
.
Australian Immunisation Handbook recommends for
people at occupational risk, Healthcare workers, to
check level of Anti-HBs (hepatitis B surface antibody)
after the vaccination course. This is to assess for
seroconversion. E.g., Check one month after dose 3.
Further vaccination (up to 6-doses) may be
recommended as per
Australian Immunisation
Handbook if immunity is not obtained post dose 3.
Candidates who are hepatitis B non-responders (after
6 dose vaccination course) can be referred to SCHHS
infectious diseases clinic for intradermal vaccination
review.
6.
Documented evidence that an individual is not
susceptible to hepatitis B infection may include
serology testing indicating a hepatitis B core
antibody (Anti-HBc / HBcAb), or a documented
history of past hepatitis B infection. Prospective
workers (including students and volunteers) who are
hepatitis B antigen positive do not have to disclose
their hepatitis B infection status but must comply
with the
SCHHS Infected Health Care Workers:
Management of Blood Borne Viruses procedure.
7.
Brand names of vaccines not in the Australian
Immunisation Handbook are vaccines that were
included in previous immunisation schedules.
Internationally administered vaccine may have a
different brand name.
8.
Pre-offer of employment/ engagement requires
evidence of completed COVID-19 vaccine course
within recommended schedule.
